

How to Cite | Publication History | PlumX Article Matrix
R. Tamilchudar1* , B. Sendilkumar2 and K. Srividhya3
, B. Sendilkumar2 and K. Srividhya3
1Department of Public Health, School of Allied Health Sciences VMRF-DU, Salem, Tamil Nadu, India.
2Dean, School of Allied Health Sciences VMRF-DU, Salem, Tamil Nadu, India.
3Department of Biostatistics , School of Allied Health Sciences VMRF-DU, Salem, Tamil Nadu, India.
Corresponding Author E-mail:fahsvmrf@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/3295

ABSTRACT: A prevalent and dangerous medical condition that hurts a person's feelings, thoughts, and behavior is depression. As stated by WHO, “A typical symptom of depression is a loss of interest in activities that one usually enjoys and a persistent sadness that lasts for at least two weeks, making it difficult to carry out daily activities”. Additional symptoms include low energy, altered appetite, increased or decreased sleep, anxiety, difficulty concentrating, difficulty making decisions, restlessness, feelings of guilt, hopelessness, or unworthiness, and suicidal thoughts. In 2015, it was projected that there were over 300 million cases of depression worldwide or 4.3% of the world's population. As per the 2015-2016 National Mental Health Survey (NMHS), one in every 20 Indians has depression, and approximately 15% of adult Indians require active care for one or more mental health conditions. According to statistics, depression accounts for 7.5% of all years survived with an infirmity in 2015, making it the leading cause of disability worldwide. When depression reaches its worst, it can result in suicide, which claims the lives of over 800,000 individuals annually. For those aged 15 to 29, it is the second most common cause of death1. Allied Health Sciences Students as primary health care workers/professionals will play an important part in identifying the symptoms of depression if any in a patient even when they come for a different health issue.
KEYWORDS: Awareness; Allied Health Sciences (AHS) students; Attitude; Depression; Diagnosis; Knowledge
Download this article as:| Copy the following to cite this article: Tamilchudar R, Sendilkumar B, Srividhya K. Assessment of Knowledge and Attitude of Allied Health Sciences Students Regarding Depression Among Patients. Biotech Res Asia 2024;21(3). |
| Copy the following to cite this URL: Tamilchudar R, Sendilkumar B, Srividhya K. Assessment of Knowledge and Attitude of Allied Health Sciences Students Regarding Depression Among Patients. Biotech Res Asia 2024;21(3). Available from: https://bit.ly/3zuARZb |
Introduction
A common and hazardous health condition that hurts a person’s feelings, thoughts, and behavior is depression. Additionally, medical disorders can resemble depressive indications, so it’s critical to rule out other possible medical causes. Based on the WHO, depression is a widespread ailment that lasts for at least two weeks and is distinguished by a tenacious sense of despondency and a decline of enthusiasm in pursuits that one usually enjoys. It also makes it difficult to do daily tasks. Additional symptoms include low energy, altered appetite, increased or decreased sleep, anxiety, difficulty concentrating, difficulty making decisions, agitation and guilt-ridden sentiments, hopelessness, otherwise unworthiness, as well as suicide ideas. In 2015, it was assessed that over 300 million individuals worldwide suffered from depression or 4.3% of the world’s populace. The NMHS of 2015-16 in India showed that one in every 20 Indians has depression and that close to 15% of adult Indians require vigorous treatment for one or more mental health problems. Depression is the primary reason for disability worldwide, secretarial for 7.5% of all years surviving with impairment in 2015. At its most severe, depression may chief to suicide; over 800,000 individuals pass away by suicide each year. It’s the 2nd biggest reason for morbidity among those aged 15 to 29 years. Allied Health Sciences Students as primary health care workers/professionals will play an important part in identifying the symptoms of depression if any in a patient even when they come for a different health issue. They have the vital role of eliciting a complete history that would consist of the presence or diagnosed medical illness like Thyroidism, Vitamin deficiencies, Neuro problems, and others that might correlate with Depression and also might be capable of identifying depression based on simple questions and behavior observations.
Rationale
Allied Health Sciences students should develop a good knowledge to identify, Diagnose, and refer cases of depression among patients.
Aim
To evaluate the knowledge and attitude about depression amongst Allied Health Sciences students.
Objectives
To evaluate the knowledge and attitude of Allied Health Sciences students regarding depression among patients.
To understand if any special training for diagnosis of Depression is required for Allied Health Sciences Students.
Materials and Methods
Study Design
The study design employed was cross-sectional.
Study location
The study was carried out in college students pursuing Allied Health Sciences.
Inclusion Criteria
Participants are students pursuing 4 Year Degree program in AHS like Bachelor of Science in Anesthesia Tech., Cardiac Tech., Perfusion Tech., Operation Theatre Tech., Physician Assistant, Medical Lab Tech., Radiography, Nuclear Medicine Tech., Neuro Science Tech., Renal Dialysis Tech., Trauma Care Management, and B. Optometry. This study includes individuals above 17 years of age, of both genders.
Exclusion Criteria
Any participant above 24 years of age. Any participant who has completed other degrees before Allied Health Sciences. Any student undergoing medical treatment for any health issues.
Period of Study
August 2022 to October 2022.
Sample Size Calculation
To help with the process of determining the sample size, n, of our specified data populace, a literature search is conducted. The appropriate sample size, n = 370, for the total population of 10,000 Allied Health Sciences students, is determined by the Krejcie and Morgan table of sample sizes.
Study Technique
Face-to-face interview method (Standardized Questionnaires were utilized) Study tools: A Module on the basics of depression like signs and symptoms, psychotherapy, and pharmacological treatment is given to the student and following completion of the module the students are given a questionnaire that is utilized to get the information among AHS students which has information about Demographic data, Questions to assess Knowledge and Attitude about depression among patients based on the module. The questionnaire administration took approximately 10 to 15 minutes of study participants’ time.
Participants’ Knowledge will be scored using these criteria
The knowledge section consisted of 14 knowledge-based questions. After reading the passages, participants were asked to choose their favorite out of three based on comprehension and knowledge. Based on their accurate and inaccurate responses, the participants’ responses were rated. Each incorrect answer was assigned a score of zero, while each correct answer received a score of one. The scoring criteria were based on previous research by Tyler et al.2 & Jerger et al.3. The following standards were used to assess participants’ level of knowledge:
| Score | Knowledge |
| 0–7 Correct answers (<50%) | Inadequate knowledge |
| 8–14 Correct answers (>50%) | Adequate knowledge |
Participants’ Attitude will be scored using these criteria:
The attitude section included 15 attitude-based questions to assess participants’ attitudes toward depression among patients. Participants were instructed to read all of the positively keyed statements and indicate whether they agreed, disagreed, or were unsure about them. The criteria for evaluating participants’ attitudes were as follows:
| Score | Attitude |
| Score 0–20 (<40%) | Negative attitude |
| Score 21–30 (41–60%) | Neutral attitude |
| Score 31–50 (61 to 100%) | Positive attitude |
Review of Literature
A study on methodical analysis for the Global Burden of Disease Study 2015 had shown that depressive mental illness was assessed to be the 3rd foremost reason for infirmity universally among the 310 diseases that caused disability4. Utilizing data composed in the National Institute of Mental Health Epidemiologic Catchment Zone Platform, It was scrutinized that the described age at onset of chief miserable illness is bimodal and maximum individuals initially appearing in their late teens, using life table survival methods as shown by Burke KC et al.5. The Baltimore Epidemiologic Catchment Zone Follow-up study by Eaton WW et al. has shown that the second peak of chief depressive disorder which is bimodal and has the initial onset in twenties occurs in the fifties6. Kessler RC et al. The epidemiology of main depressive disorder: results from the National Comorbidity Survey Replication have clinched that Chief depressive disorder is a common disorder, broadly dispersed in the population, and usually related with considerable indication severity and role injury. The emphasis on screening and expanding therapy must be supported by a similar emphasis on improving treatment quality. Females are double as likely to suffer from depression as males. According to Weissman MM et al., the major peril elements for the improvement of chief depressive disorder comprise being divorced or separated8, having previously experienced depression, having elevated levels of stress, having a history of trauma, and having a history of major depressive disorder in first-degree relatives, and the reports of American Psychiatric Association9. A study to determine KAP about Mental Health Challenges among Healthcare Students of a Private University was conducted and the results showed that Knowledge from the Faculty of Medicine was sufficient compared to that of the Faculty of Pharmacy and Dentistry10. RG Frank has pointed out in his study that numerous studies have shown deficiencies in the primary care sector’s ability to manage depression effectively and also has shown that 60% of mental health services are delivered in primary care settings11. Ahmedani BK et al. conducted a study in the US on racial/ethnic variances in medical care visits made before suicide attempts. According to the study, 64% of individuals who tried suicide saw a doctor within four weeks before the attempt, and 38% of those who did so within the week prior. Most of these patients attended a primary care facility12.
Results
Table 1: Responses by Allied Health Sciences Students towards Knowledge about depression among patients.
| S.No | Knowledge-based Questions(Standardized Questionnaire) | Don’t Known (%) | Non (%) | Yesn (%) |
| 1 | Do you know anything about depression? | 45 (5) | 219 (25) | 604 (70) |
| 2 | Do you view depression as a health issue? | 27 (3) | 296 (34) | 545 (63) |
| 3 | Depression affects people of any age group. | 65 (7) | 382 (44) | 421 (49) |
| 4 | Witchcraft, charms, or bad spirits are not the cause of depression. | 189 (22) | 207 (24) | 472 (54) |
| 5 | Patients suffering from depression may experience a collapse at any time. | 77 (9) | 142 (16) | 649 (75) |
| 6 | Patients suffering from depression endanger both themselves and others. | 94 (11) | 196 (23) | 578 (67) |
| 7 | Depression can lead to suicidal ideation or attempts. | 73 (8) | 122 (14) | 673 (78) |
| 8 | Both medication and psychotherapy are effective treatments for depression. | 92 (11) | 149 (17) | 627 (72) |
| 9 | Traditional medical professionals are the best at managing depression. | 160 (18) | 200 (23) | 508 (59) |
| 10 | For the most part, conventional therapy for depression is less effective than traditional methods. | 262 (30) | 233 (27) | 373 (43) |
| 11 | Amitriptyline is a medication used to treat depression. | 223 (26) | 162 (19) | 483 (56) |
| 12 | Methotrexate is not an anti-depressant medication. | 235 (27) | 317 (37) | 316 (36) |
| 13 | One antidepressant medication is fluoxetine. | 231 (27) | 145 (17) | 492 (57) |
| 14 | One antidepressant medication is carbamazepine. | 235 (27) | 264 (30) | 369 (43) |
Awareness about Depression
70% of the respondents were aware of what is depression and 63% considered it to be a health problem.
Knowledge of the Etiology of Depression
54% are distressed that depression is triggered by sorcery or demonic entities, and 49% think depression affects only a particular age group.
Knowledge about the Symptoms and Signs of Depression
75% of respondents believed that depressed individuals might collapse at any time & 67 % realized that depressed individuals are hazardous to themselves and other people. 78% reported that melancholy may result in suicidal thoughts or actions.
Understanding how Depression is Classified and Treated
Most (72%) agreed that psychotherapy and medication may be utilized to extravagance depression whereas 59% believed that it can be treated only by traditional Doctors or healers. 43% of participants had responded that depression is better responded to conventional therapy less frequently than to traditional therapies. Almost 50% of the respondents are familiar with the anti-depression drugs. Out of 868 respondents, 13 (1.5%) respondents have complete knowledge and positive attitudes regarding depression among Allied Health Sciences Students.
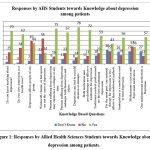 |
Figure 1: Responses by Allied Health Sciences Students towards Knowledge about depression among patients. |
Knowledge-based Percentage Analysis for the Respondents
The following table shows the percentage of knowledge regarding depression among Allied Health Sciences Students (respondents).
Table 2: Knowledge-based percentage analysis for the Respondents
| Knowledge | Respondents (n) | % |
| 50% | 79 | 9% |
| 60% | 74 | 9% |
| 70% | 58 | 7% |
| 80% | 42 | 5% |
| 90% | 39 | 4% |
| 100% | 35 | 4% |
Out of 868 respondents, 79 respondents (9%) have 50 percentage of knowledge, 74 respondents (9%) have 60 percentage of knowledge, 58 respondents (7%) have 70 percentage of knowledge, 42 respondents (5%) have 80 percentage of knowledge, 39 respondents (4%) have 90 percentage of knowledge and 35 respondents (4%) have 100 percentage of knowledge.
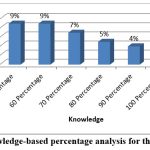 |
Figure 2: Knowledge-based percentage analysis for the Respondents |
The following table demonstrates the below 50 percent and above 50 percent of knowledge regarding depression among Allied Health Sciences Students (respondents).
Table 3: Scoring of Knowledge for the Respondents
| Knowledge | Respondents | % |
| Below 50 Percentage | 327 | 38% |
| Above 50 Percentage | 541 | 62% |
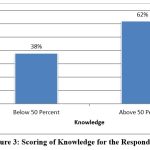 |
Figure 3: Scoring of Knowledge for the Respondents |
Table 4: Responses by Allied Health Sciences Students towards Attitudes about depression among patients
| S.No | Attitude toward causes, diagnosing and management of depression-based (Standardized) Questions | Don’t Known (%) | Non (%) | Yesn (%) |
| 1 | Most of the depressive instances I have heard about stemmed from recent tragedies. | 201 (23) | 280 (32) | 387 (45) |
| 2 | Without medicine, the majority of depressive illnesses get better. | 122 (14) | 228 (26) | 518 (60) |
| 3 | The cause of more severe depression is a biochemical imbalance. | 220 (25) | 241 (28) | 407 (47) |
| 4 | It’s challenging to distinguish between sadness and a diagnosable clinical depression that requires medical attention. | 159 (18) | 209 (24) | 500 (58) |
| 5 | Depression may be classified into two groups: depression resulting from psychological factors and depression resulting from physiological reasons. | 212 (24) | 188 (22) | 468 (54) |
| 6 | People with low endurance often turn to depression as a coping mechanism for life’s setbacks. | 166 (19) | 207 (24) | 495 (57) |
| 7 | Depressed patients are more likely to have encountered deprivation in their early lives than others. | 200 (23) | 179 (21) | 489 (56) |
| 8 | Depression is not a fixed response that cannot be changed. | 241 (28) | 200 (23) | 427 (49) |
| 9 | Becoming depressed is not a natural aspect of becoming older. | 166 (19) | 279 (32) | 423 (49) |
| 10 | The primary healthcare professional might be an excellent resource for helping depressed people. | 183 (21) | 180 (21) | 505 (58) |
| 11 | Working with patients who are depressed is difficult and time-consuming. | 192 (22) | 187 (22) | 489 (56) |
| 12 | Antidepressants are frequently effective in treating depressed individuals in general practice. | 200 (23) | 174 (20) | 494 (57) |
| 13 | Depressed persons should receive psychotherapy from an expert. | 187 (22) | 171 (20) | 510 (59) |
| 14 | For the majority of depressed individuals, psychotherapy would be more useful than medicines if it was free. | 191 (22) | 147 (17) | 530 (61) |
| 15 | The general populace discriminates against and avoids patients who suffer from depression. | 207 (24) | 235 (27) | 426 (49) |
Responses on Attitude towards Causes of Depression:
45% of participants responded that the mainstream cases of depression were the outcome of recent bad luck.
47% of respondents said that greater severity of despair is triggered by Biochemical irregularities.
56% of respondents mentioned childhood scarcity as a risk factor for depression.
Aging is a basis of depression thought 49% of participants.
Responses on Attitude to Diagnosis and Management of Depression
60% participants had responded that depression improves without medication whereas 57% believed that antidepressants help in treating depression.
60% responded that Psychotherapy would be the most beneficial treatment for depression and should be given only by a specialist.
The two types of depression that may be caused by biochemical mechanism changes or the condition caused by psychological disturbances can be differentiated in the response given by 54%.
58% of respondents felt that the feeling of misery and the gloomy condition that requires treatment cannot be differentiated by people.
57% of respondents said that persons with low endurance deal with life’s challenges by falling into depression.
49% of respondents said that depression is an ingrained reaction that cannot be altered.
58% of students believe primary care providers can assist those experiencing depression.
56% responded that dealing with depressed patients is difficult and tiresome.
49% of respondents feel that People avoid and discriminate against those who suffer from depression.
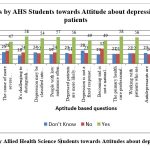 |
Figure 4: Responses by Allied Health Science Students towards Attitudes about depression among patients |
The following table demonstrates that less than 40 percent, 41 – 60, and 61 – 100 percent of attitudes regarding depression among Allied Health Sciences Students (respondents).
Table 5: Scoring of Attitude for the Respondents
| Attitude | Respondents | % |
| Less than 40 | 388 | 45% |
| 41 – 60 | 228 | 26% |
| 61 – 100 | 252 | 29% |
Out of 868 respondents, 388 respondents (45%) have scored less than 40 percentage indicating a negative attitude, 228 respondents (26%) have scored between 41 to 60 percentage indicating a neutral attitude, and 252 respondents (29%) have 61 to 100 percentage of Allied Health Sciences Students (respondents) have a positive attitude regarding depression among patients.
Discussion
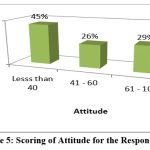 |
Figure 5: Scoring of Attitude for the Respondents |
In this study, participants had a usually high level of understanding of depression. Attitudes towards depression indicated negative replies, implying that Allied Health Science students had minimal teaching on psychological diseases. Allied Health Sciences students can play of chief role in the detection and treatment of depression. In this investigation; AHCPs share noble information about the roots of despair. In terms of depression management, the majority of people were aware of the efficacy of pharmaceutical and psychotherapeutic techniques. Additionally, the majority of participants were aware that amitriptyline, an antidepressant, is a psychotropic substance, in contrast to findings found in Nigeria14. Allied Health Students had fallacies on the perilous elements & reason of despair. Almost 45% of the respondents believed that depression is triggered by bad luck. Parallel results have been described elsewhere15,16. Previous research has demonstrated that stigma and discriminatory views toward depression might prevent depressed individuals from seeking treatment and the same responses have been received in our study too17, 18. Variations in Allied Health Sciences students’ sights on depression might be significantly impacted by communal and ethnic factors19. The mainstream Allied Health Sciences students felt uncomfortable or it was tough to work with patients who were depressed. This is reliable with past studies20. 58% of Allied Health Sciences students reported not having trouble discriminating grief from a clinical depressive state which is crucial therapy. Our outcomes are similar to a study amid GPs in France15 but different from GPs in Brazil21. The mainstream of the defendants desired that depressed patients be handled by experts. Other investigations had similar results 22,19,23,24.
Because Allied Health Sciences students cannot diagnose and provide appropriate management alternatives, they prefer to have depression managed by mental health experts. As previously established, difficulties in the diagnosis and treatment of depression include time limits, limited abilities, and training 13, 19. A study conducted in the UK by Haddad et al. found that if nurses in common practice received proper psychological fitness training; they might deliver stronger behavioural health amenities 25, ancillary to the results of other studies 26,14,27,28.
The following limitations applied to the study. It utilized a non-probability sampling technique & was completed among Allied Health Science students of a particular college and hence is not a very good representation of the whole population of Allied Health Science students. We didn’t assess the validity that includes common test result features, internal reliability, and factor structure of the questionnaire nor its psychometric possessions. However, using this questionnaire gave us the chance to relate the results in African sets & elsewhere which applied a similar tool. Thus, it may be necessary to conduct broader research among Allied Health Sciences students from different colleges in various regions of the nation. There was recollection prejudice, as the mainstream of people who had received mental health training were unable to accurately guesstimate the period of training or the type of mental illness examined. These precincts must be noted when inferring the findings. Despite these confines, this paper presents fresh data on the knowledge and attitudes of Allied Health Science students on depression in patients.
Implications
Instructive interference initiatives in sectors of psychological well-being to progress the knowledge and attitudes of Allied Health Sciences students toward depression among patients are paramount.
If this is implemented, Allied Health Sciences students will be additionally self-assured in dealing with depressed patients.
Prior research has indicated that sustained medical education is linked to enhanced referral, identifying, and treating people with depression.
Conclusion
Allied Health Science students have insufficient Knowledge but a positive attitude about the awareness, causes, diagnosis, and management of despair among patients. There were few choices for managing depression.
Allied Health Science students had inadequate training in mental health.
Suggests that the curriculum of Allied Health Science should include subjects relevant to knowing cognitive illnesses.
Acknowledgement
The authors would like to thank the authors of the literacy sources cited in this article.
Conflict of Interest
The authors do not have any conflict of interest.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Microsoft Excel was utilized to enter and analyze the data. SPSS software was used to carry out the statistical analysis. The manuscript incorporates and uses all data examined throughout this study.
Ethical Statement
This study was agreed upon by the Ethical Committee of Vinayaka Missions Kirubananda Variyar Medical College & Hospital, VMRF-DU, Salem, Tamil Nadu, India. Written informed consent was acquired from every individual involved.
References
- Bhargava, I., and Mor, N. Mental Health in India: The Path Forward, 2024.
- Tyler, D. C., Tu, A., Douthit, J., and Chapman, C. R. Toward validation of pain measurement tools for children: a pilot study. Pain, 1993, 52(3), 301-309.
CrossRef - Jerger, J., Johnson, K., and Jerger, S. Effect of Response Criterion on Measures of Speech: Understanding in the Elderly. Ear and hearing, 1988, 9(2), 49-56.
CrossRef - Feigin, V. Global, regional, and National Incidence, prevalence, and years lived with disability for 310 acute and chronic diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015, 2016.
- Burke, K. C., Burke, J. D., Regier, D. A., and Rae, D. S. Age at the onset of selected mental disorders in five community populations. Archives of general psychiatry, 1990, 47(6), 511-518.
CrossRef - Eaton, W. W., Anthony, J. C., Gallo, J., Cai, G., Tien, A., Romanoski, A., and Chen, L. S. Natural history of Diagnostic Interview Schedule/DSM-IV major depression: The Baltimore epidemiologic catchment area follow-up. Archives of general psychiatry, 1997, 54(11), 993-999.
CrossRef - Kessler, R. C., Berglund, P., Demler, O., Jin, R., Koretz, D., Merikangas, K. R., and Wang, P. S. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). Jama, 2003, 289(23), 3095-3105.
CrossRef - Weissman, M. M., Bland, R. C., Canino, G. J., Faravelli, C., Greenwald, S., Hwu, H. G., and Yeh, E. K. Cross-national epidemiology of major depression and bipolar disorder. Jama, 1996, 276(4), 293-299.
CrossRef - Dsm, I. V. Diagnostic and statistical manual of mental disorders. Washington, DC: American psychiatric association, 1994, 968, 33-36.
- Iqbal, M. Z., Rathi, R., Prajapati, S. K., Qing, M. S. Z., Pheng, T. S., Kee, H. W., and Iqbal, M. S. Knowledge, attitude, and practice about mental health challenges among healthcare students of a private university. Journal of Pharmacy and Bio allied Sciences, 2021, 13(1), 136-142.
CrossRef - Frank, R. G., Huskamp, H. A., and Pincus, H. A. Aligning incentives in the treatment of depression in primary care with evidence-based practice. Psychiatric Services, 2003, 54(5), 682-687.
CrossRef - Ahmedani, B. K., Stewart, C., Simon, G. E., Lynch, F., Lu, C. Y., Waitzfelder, B. E., and Williams, K. Racial/ethnic differences in health care visits made before suicide attempt across the United States. Medical care, 2015, 53(5), 430-435.
CrossRef - Chen, S., Conwell, Y., Xu, B., Chiu, H., Tu, X., and Ma, Y. Depression care management for late-life depression in China primary care: Protocol for a randomized controlled trial. Trials, 2011, 12, 1-14.
CrossRef - Odejide, A. O., Morakinyo, J. J., Oshiname, F. O., Omigbodun, O., Ajuwon, A. J., and Kola, L. Integrating mental health into primary health care in Nigeria: management of depression in a local government (district) area as a paradigm. Seishin shinkeigaku zasshi= Psychiatria et neurologia Japonica, 2002, 104(10), 802-809.
- Norton, J. L., Pommié, C., Cogneau, J., Haddad, M., Ritchie, K. A., and Mann, A. H. Beliefs and attitudes of French family practitioners toward depression: the impact of training in mental health. The International Journal of Psychiatry in Medicine, 2011, 41(2), 107-122.
CrossRef - Haddad, M., Waqas, A., Qayyum, W., Shams, M., and Malik, S. The attitudes and beliefs of Pakistani medical practitioners about depression: a cross-sectional study in Lahore using the Revised Depression Attitude Questionnaire (R-DAQ). BMC psychiatry, 2016, 16, 1-11.
CrossRef - Mansouri, N., Gharaee, B., Shariat, S. V., Bolhari, J., Yousefi Nooraie, R., Rahimi-Movaghar, A., and Alirezaie, N. The change in attitude and knowledge of health care personnel and general population following trainings provided during integration of mental health in Primary Health Care in Iran: a systematic review. International Journal of Mental Health Systems, 2009, 3, 1-7.
CrossRef - Kobau, R., Zack, M. M., Luncheon, C., Barile, J. P., Marshall, C., Bornemann, T., and Morales, D. S. Attitudes toward mental illness: Results from the behavioral risk factor surveillance system, 2012.
- Ndetei, D. M., Khasakhala, L. I., Mutiso, V., and Mbwayo, A. W. Knowledge, attitude and practice (KAP) of mental illness among staff in general medical facilities in Kenya: practice and policy implications: original. African journal of psychiatry, 2011, 14(3), 225-235.
CrossRef - James, B. O., Jenkins, R., and Lawani, A. O. Depression in primary care: the knowledge, attitudes and practice of general practitioners in Benin City, Nigeria. South African Family Practice, 2012, 54(1), 55-60.
CrossRef - Botega, N. J., and Silveira, G. M. General practitioners’ attitudes towards depression: A study in primary care setting in Brazil. International Journal of Social Psychiatry, 1996, 42(3), 230-237.
CrossRef - Mbatia, J., Shah, A., and Jenkins, R. Knowledge, attitudes and practice pertaining to depression among primary health care workers in Tanzania. International Journal of Mental Health Systems, 2009, 3, 1-6.
CrossRef - Ohtsuki, T., Kodaka, M., Sakai, R., Ishikura, F., Watanabe, Y., Mann, A., and Inagaki, M. Attitudes toward depression among Japanese non-psychiatric medical doctors: a cross-sectional study. BMC research notes, 2012, 5, 1-8.
CrossRef - Street, A., and Center, A. General practitioners knowledge and attitude towards anxiety and depression in Abu Dhabi. The Middle East Journal, 2006, 4.
- Haddad, M., Walters, P., and Tylee, A. District nursing staff and depression: a psychometric evaluation of Depression Attitude Questionnaire findings. International Journal of Nursing Studies, 2007, 44(3), 447-456.
CrossRef - Thapa, P., Rawal, N., and Bista, Y. A study of depression and anxiety in cancer patients. Nepal Medical College journal: NMCJ, 2010, 12(3), 171-175.
- Dowrick, C., Gask, L., Perry, R., Dixon, C., and Usherwood, T. Do general practitioners’ attitudes towards depression predict their clinical behaviour?. Psychological medicine, 2000, 30(2), 413-419.
CrossRef - F Furegato, A. R., Ferreira da Silva Candido, M. C., & Lobo da Costa Jr, M. (2009). Comparing knowledge and opinions on depression among nurses in the health services. Revista de Salud Pública, 11, 200-211.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



