

Manuscript accepted on : 25-09-2024
Published online on: 05-10-2024
Plagiarism Check: Yes
Reviewed by: Dr. Rajat Goyal
Second Review by: Dr Moumita Hazra
Final Approval by: Dr. Chateen Izaddin Ali Pambuk
A Step Towards Combating Antimicrobial Resistance: Global Prescriptive and Programmes – A Review
Vatsa Kapadia1, Ashish Wadhwani1*, Rihana Begum2, Sivasankaran Ponnusankar2 , Praveen Mohadeb3, Medha Gujadhur3 and Piyush Kumar4
1Department of Pharmaceutical Biotechnology, JSS College of Pharmacy, JSS Academy of Higher Education and Research, Ooty, Nilgiris, Tamil Nadu, India
2Department of Pharmacy Practice, JSS College of Pharmacy, JSS Academy of Higher Education and Research, Ooty, Nilgiris -643001, Tamil Nadu, India
3Faculty of Health Sciences, School of Pharmacy, JSS Academy of Higher Education and Research, Vacoas, Mauritius
4JSS College of Pharmacy, Najwal, Jammu, Jammu and Kashmir, India
Corresponding Author E-mail: dradwadhwani@jssuni.edu.in
DOI : http://dx.doi.org/10.13005/bbra/3271

ABSTRACT: Antimicrobial resistance is one of the pandemic concerns that lead to morbidity and mortality. The unregulated use of antibiotics results in strains and genes which are resistant to antibiotics. In general, mutations resulting in antimicrobial resistance alter the antibiotic action via one of the mechanisms: modifications of the antimicrobial target; a decrease in the drug uptake; activation of efflux mechanisms to extrude the harmful molecule, or; global changes in important metabolic pathways via modulation of regulatory networks. Furthermore, a shortage of financing, as well as tight rules governing the production and marketing of new pharmaceutical treatments, contribute to an increase in antimicrobial resistance. Specialized organizations concerned with worldwide public health, such as the United Nations (UN) and the World Health Organization (WHO), have identified antibiotic resistance as an issue that necessitates globally coordinated efforts and the utmost care. The WHO has founded many national and international surveillance programmes across various countries. Some of the Indian government's programs are the Red Line Initiative, Chennai Declaration, Antimicrobial Stewardship Program, National AMR Containment Program, National Health Policy, National Action Plan on NAP-AMR antimicrobial resistance, etc. These monitoring programmes' findings clearly indicate that sensible antibiotic usage, appropriate antibiotic knowledge, awareness and the development of novel medications will all aid us in combating the antimicrobial resistance issue. This review article discusses worldwide programmes and activities to combat developing and growing antimicrobial resistance that are being implemented by various Indian states and in Mauritius.
KEYWORDS: Antibiotics; Antimicrobial resistance; Microorganisms; Policies; Programmes
Download this article as:| Copy the following to cite this article: Kapadia V, Wadhwani A, Begum R, Ponnusankar R, Mohadeb P, Gujadhur M, Kumar P. A Step Towards Combating Antimicrobial Resistance: Global Prescriptive and Programmes – A Review. Biotech Res Asia 2024;21(3). |
| Copy the following to cite this URL: Kapadia V, Wadhwani A, Begum R, Ponnusankar R, Mohadeb P, Gujadhur M, Kumar P. A Step Towards Combating Antimicrobial Resistance: Global Prescriptive and Programmes – A Review. Biotech Res Asia 2024;21(3). Available from: https://bit.ly/4dDAnOq |
Introduction
Antimicrobial resistance (AMR) has emerged as one of this century’s major health problems and has elevated the need to prevent and treat infections caused by virus, bacteria, fungi and parasites. One of the reasons being, those organisms are no longer susceptible to the medicines used to treat them. Most cases involving bacterial infections established antimicrobial resistance to even the newer antibiotics in recent decades posing an emergency problem that needs to be addressed appropriately. This growing resistance is the result of inappropriate antibiotic usage in people, veterinary medicine, and agriculture as a result of accessible and uncontrolled availability, particularly in poor nations. Antibiotic resistance can occur intentionally (by transferring resistance gene) and naturally1.
The emergence and increasing prevalence of microbial resistance to antimicrobial medicines is one of the major global health issues 2. Worldwide drug-resistant illnesses are a major source of unrest. Methicillin-resistant Staphylococcus aureus (MRSA) is a single organism that kills approximately 19,000 more people yearly than combined homicide, emphysema, HIV/AIDS, and Parkinson’s disease combined3. Ninety-nine thousand Americans die from nosocomial infections (HAIs) each year 4, the great majority of which are caused by microorganisms resistant to antibacterial agents (antibiotics). Only two common medical conditions, pneumonia and sepsis, claimed the lives of nearly 50,000 Americans in 2006, yet the US health care system spent more than $8 billion on these treatments5. According to a recent survey, in more than 1,000 intensive care units across 75 nations, half of the patients had an infection, and the risk of an infection-related hospital death was twice that of an uninfected patient6-9.
Due to restricted treatment choices, resistant bacteria (RB) can cause severe illnesses that are growing more difficult to cure. Multiple-resistant (MDR) bacteria, which are characterised as strains resistant to at least one agent from three or more antibiotic groups, are the most life-threatening type of resistant bacteria. These multiple-resistant (MDR) bacteria strains pose a severe concern to humanoid well-being, particularly in clinics where they can result in nosocomial infections10. Pseudomonas aeruginosa, Acinetobacter baumannii, Escherichia coli, Klebsiella pneumoniae, vancomycin-resistant Enterococci (VRE), methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant S. aureus (VRSA), and extensively drug-resistant (XDR) Mycobacterium tuberculosis bacteria are among the many multi-resistant bacteria that are extremely difficult to handle.1
“Antibiotic resistance” is described as “a bacterial characteristic that prevents the inhibitory effects of antibiotics to which it was earlier sensitive, allowing it to survive despite antimicrobial exposure.” 11. Antibiotic Resistant Microorganisms have been dubbed “Nightmare Bacteria” because they cause unanticipated great harm to the world’s people. In most cases of long-term and costly treatments with antibiotic-resistant infections; even prolonged hospitalization and regular doctor visits are required to decrease the mortality rate due to infections that can be easily treated with antibiotics. A 2013 study by the Centre for Disease Control and Prevention (CDC) recommended four core actions, such as avoiding infection and increasing resistance; monitoring resistant bacteria; enhancing the antibiotic use which are existing and encouraging new development of antibiotics; and developing new diagnostic methods for resistant bacteria (Figure – 1)12. This article is an overview of the antimicrobial resistance, its mechanism, causes, and programs and initiatives conducted to overcome this crisis.
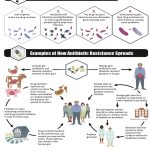 |
Figure 1: The figures show antibiotic resistance and its spread. The resistance is usually produced by the easy use of antibiotics13. Click here to view Figure |
Mechanism of Antimicrobial Resistance
Antimicrobial drugs are divided into different categories based on the mechanism of their activity. The main categories are: drugs that prevent the synthesis of cell walls, alter the membrane of the cell, stop protein synthesis, inhibit the merger of nuclei acids and inhibit bacterial metabolic pathways. Table 1 represents antimicrobial drugs from each of these groups. It was realistic that everybody had greater control over the microorganisms with these kinds of large spectrum of mechanisms. Unfortunately, inadequate handling of antimicrobial drugs has helped to contribute to the enormous challenge of rising resistance that everyone still faces. Reasons that have contributed to the increasing issue of resistance include: increased use of antimicrobial drugs and excessive dosage of antimicrobial drugs 14. Doctors can misuse various popular antimicrobial drugs because the choice of drugs is based on a mixture of low cost and low toxicity 15. Antimicrobials, such as the original prescribing of a broad-spectrum drug that is inappropriate or eventually determined to be inadequate for the organism(s) causing the infection, can also be inappropriately administered16. The improper use of antimicrobial drugs results in the production of resistant species. In addition, previous use of antimicrobial medications places a patient at risk with a drug-resistant organism infection, and the patients most often afflicted with resistant bacteria are those with the greatest sensitivity to antimicrobials.
Table 1 : Mechanism of action of certain antimicrobial drugs and their target sites14
| Drug Class | Target | Mechanism of Action |
| β-lactams: penicillins, cephalosporins, monobactams, carbapenems | Penicillin-binding proteins | Inhibition of cell wall biosynthesis |
| Glycopeptides | Peptidoglycan subunits | |
| Bacitracin | Peptidoglycan subunit transport | |
| Aminoglycosides, tetracyclines | 30S ribosomal subunit | Inhibition biosynthesis of proteins |
| Macrolides, lincosamides, chloramphenicol, oxazolidinones | 50S ribosomal subunit | |
| Polymyxin B, colistin, daptomycin | Lipopolysaccharide, inner and outer membranes | Disrupt membranes |
| Rifamycin | Ribonucleic acid (RNA) | Inhibition of nucleic acid synthesis |
| Fluoroquinolones | Deoxyribonucleic acid (DNA) | |
| Sulphonamides, trimethoprim | Folic acid synthesis enzyme | Antimetabolites |
| Isonicotinic acid hydrazide | Mycolic acid synthesis enzyme | |
| Diarylquinoline | Mycobacterial ATP synthase | Mycobacterial adenosine triphosphate (ATP) synthase inhibitor |
AMR Causes
Antibiotic overuse and misuse.
Inadequate product production by the pharmaceutical industry due to the challenging regulatory conditions and raising financial incentives13.
Use of antibiotics in animal feed to avoid, monitor and treat animal diseases (e.g., Streptomycin is used to prevent diseases caused by Erwiniaamylovora in apple and pear trees)17.
Intrusive surgical procedures, patients who are immunocompromised, and elderly.
Lack or incorrect antibiotic awareness.
Self-medication
In growth promotion of the food producing animals18.
Bacteria-resistant strains spread in the environment from person to person or from non-human origin (due to the release by humans of incompletely metabolized antibiotics and the disposal of unused antibiotics)19.
Without antibiotics, the most advanced surgical techniques, transplants, developments in neonatal drug and developments in chemotherapy for cancer patients may not have existed20. Apart from vaccination, few experimental findings have had such a wide-ranging impact on the delivery of healthcare. And yet we have entered a point today where drug-resistant bacteria face significant fears to humanity. There was still this danger on the horizon. Sir Alexander Fleming noticed as early as 1943 that the bacteria were conditioned to withstand penicillin, but relatively little has been done over the past few decades to address the emerging challenge of drug resistance21. Measures such as antibiotic organization and infection controller have been introduced, but these steps have mostly been taken locally and periodically as a reactive tactic rather than as part of any tactical planning and visualization22. Regardless, these measures have just given transitory advantage. The logical progressions regarding disclosure of new particles and targets have experienced much more dormancy and furthermore from absence of course.
Antimicrobial Stewardship Programs
In order to minimize the spread of antimicrobial resistance, individual patient treatment and reduce hospital costs, antimicrobial stewardship initiatives in the healthcare sector aim to increase antimicrobial prescribing. Antimicrobial management systems are more critical than ever in ensuring the continued effectiveness of available antimicrobials, with antimicrobial resistance growing worldwide and few new agents in growth. The strategy for antimicrobial administration projects should be focused on the best-established understanding of the relation between antimicrobial usage and obstruction. These programs should be headed by multidisciplinary groups of irresistible ailments doctors, medicinal drug experts, clinical microbiologists, and management practitioners made up of enticing illnesses and should be successfully maintained by emergency clinic chairmen23.
Antimicrobial stewardship corresponds to the ten best public health system:
At the community, regional, state, and national levels, antimicrobial susceptibility patterns and antimicrobial use trends are monitored and detected.
Antimicrobial vulnerability monitoring at the community, regional, state, and national levels.
The transmission of knowledge through education motivates individuals, healthcare professionals, and other entities regarding optimal antibiotic usage.
Collaborate with community groups, such as hospitals, long-term care institutions, and healthcare systems, to promote antimicrobial stewardship practises across areas, particularly with common patient populations.
Identify and broadly distribute best practises and policies in AMS.
Provide advocacy efforts to promote policies that will enhance patient safety, limit exposure, and prevent the spread of antibiotic-resistant diseases.
To improve AMS across areas, establish connections between healthcare institutions.
Ascertain that an effective ASP is in place at healthcare institutions.
In order to enhance healthcare facilities, monitor and assess ASP.
The development of novel research solutions to AMS implementation challenges24.
Action to Combat Antibiotic Resistance
The issue of global antimicrobial resistance is on the rise and is connected to increased morbidness and prevalence in the health care sector. The development of antibiotic resistance to multiple environmental condition and the expansion of superbugs renders successful prevention methods much more complicated. In order to control and avoid antimicrobial resistance, local, national and international interventions have been recommended. The most suggested interventions are controls on over-the-counter antibiotic supply, fair use of antimicrobials, enhancing infection prevention and management, and improving hand hygiene. The need for a comprehensive understanding of the mechanisms of resistance and progress of novel medicines and vaccines is of utmost importance. The battle against antimicrobial resistance requires an interdisciplinary, cooperation, and regulatory strategy25.
 |
Figure 2: The figure shows various actions and parameters to Combat Antibiotic ResistanceClick here to view Figure |
Initiations of Who
WHO’s policies
WHO has released a strategy package to challenge antimicrobial resistance on World Health Day 2011.This package represents the serious steps that governments and health departments need to take to stimulate variety among all investors 26.
Engage with transparency and civil society participation in a robust, funded national strategy.
Strengthen monitoring and laboratory capabilities.
Ensuring unrestricted access to critical quality guaranteed pharmaceutical goods.
Regulate and encourage the rational use of drugs, including in animal raising, and ensure adequate care for patients.
Enhance infection prevention and control (IPC).
Promoting creativity and R&D for new instruments.
Global Action Plan
In May 2015, at the WHA (World Health Assembly), a worldwide antimicrobial resistance action plan was acknowledged. The Global Action Plan’s objective is to oversee the use of safe and effective medications for the prevention and treatment of infectious diseases. It has 5 tactical goals 27:
Boost recognition and knowledge of antimicrobial resistance.
Improving monitoring and research.
To minimize the rate of infection.
To streamline the use of antimicrobial drugs.
Ensuring sustainable investments to tackle antimicrobial resistance.
At the United Nations General Assembly in New York in September 2016, heads of state adopted a political statement that demonstrated the global community’s commitment to addressing the primary causes of antimicrobial resistance in a variety of industries, with a focus on human health, animal health, and husbandry. World Health Organization (WHO) promotes the implementation of national antimicrobial resistance action plans by Member States, based on the Global Action plan.
World Antimicrobial Awareness Week (WAAW)
World Antimicrobial Awareness Week (WAAW), which has been recognised annually since 2015, is a global initiative aimed at increasing global awareness of antimicrobial resistance and encouraging best practices among policy makers, health professionals and the public to prevent the further increase and spread of drug-resistant infections. Antimicrobial medicines are important for combating human, animal and plant infections. Antibiotics, antifungals, antiprotozoal medications, and antivirals are included. Every year, World Antimicrobial Awareness Week (WAAW) is observed from November 18 to November 24. The 2020 campaign, which reflected the wider range of drug-resistant illnesses, replaced the initial slogan, “Antibiotics: Handle with Care,” with “Antimicrobials: Handle with Care”28.
Global Antimicrobial Resistance Surveillance System (GLASS)
The Global Antimicrobial Resistance Surveillance System (GLASS) was developed in October 2015 to support the Global Antimicrobial Resistance Action Plan. The goal is to encourage global surveillance and investigate to improve the antimicrobial resistance (AMR) knowledge base and to help guide decision-making and accelerate national, geographical and world-wide action[29]. The prime scope of GLASS are:
Encourage national monitoring frameworks and harmonized global requirements;
Evaluation the degree and pressure of AMR world-wide across selected metrics;
Analysis and reporting of world-wide data on AMR on a periodic basis;
Detect evolving resistance and its dissemination internationally;
Informing the introduction of tailored programmes of prevention and regulation; and
Assessing the effects of treatments.
Global Antibiotic Research and Development Partnership (GARDP)
Established in 2016 by the WHO and the Drugs for Neglected Disease initiative (DNDi), GARDP is an integral component of the world-wide Antimicrobial Resistance Action Plan of the WHO. GARDP was developed to ensure that anyone who wants antibiotics requires appropriate and fair care anywhere they live and plans to introduce five novel drugs treatments to tackle drug-resistant infections by 2025, directing on sexually transmitted infections, sepsis in new-borns and infections in hospitalized adults and infants30.
Interagency Coordination Group on Antimicrobial Resistance (IACG)
IACG was founded by the Secretary-General of the United Nations to foster cooperation among global administrations and to safeguard successful worldwide action against this challenge to health protection. The IACG is co-chaired by the Deputy Secretary-General of the United Nations and the Director-General of the World Health Organisation (WHO) and is made up of high-level members of the different United Nations institutions, other global organisations and individual professionals from various sectors31.
WHO has also introduced Tuberculosis (TB), HIV and Malaria Surveillance Systems for Strong Drug Resistance. After the start of HIV surveillance programs in 2005, the TB surveillance system has been developed in about 188 countries. Such services have the main functions of preparing diagnostics, designing treatment regimens and tracking management interventions32.
Programms by Centers For Disease Control and Prevention
CDC is a leader in fighting global antimicrobial resistance threat. Through its furious action, it works independently and in partnership, and provides a resourceful antimicrobial resistance solution to enable the country to exhaustively counter the crisis. It offers financial assistance to some fifty state and six local health departments and Puerto Rico, and favours changing the battle between antimicrobial resistance and the environment. The AR Investment Map (2018) is one such program [33].
Antimicrobial Resistance Investment 2018 Map
CDC ‘s AR investment map contains the latest data released to strengthen efforts to protect people from antibiotic resistance in the U.S. and even outside the world. It attributes to the global and extramural alliance to recognize and execute novel solutions to protect people from the antibiotic resistance crisis.
National Antimicrobial Resistance Monitoring System (NARMS)
It is a United State (US) community health monitoring scheme designed to track antimicrobial resistance in food-borne bacteria and enteric bacteria mainly from the sources of humans, retail foods, and food animals. It functions in collaboration with the US Centre for Disease Control and Prevention (US CDC), US FDA (US Food and Drug Administration), USDA (US Department of Agriculture), and other agencies of state and local health. It initially started with human surveillance in the year 1996 in fourteen areas, and later developed throughout the country in 2003 [34].
NARMS reports are released annually, consisting of the number data, the types of isolates of the bacteria that have acquired their antimicrobial resistance and the antimicrobial resistance drifts. The report is a compilation of Centre for Disease Control and Prevention (CDC) reports on human isolates, US Food and Drug Administration’s retail meat isolates, US Department of Agriculture’s Animal isolates, and FDA’s Interagency Executive report. Minimum inhibitory concentration determines antibiotic susceptibility of the isolates. At present, eighteen antibiotic agents are regularly evaluated by CDC NARMS [35].
NARMS focuses mainly on identifying and characterizing non-typhoidal salmonella and Campylobacter two main foodborne diseases that spread bacteria in the United States. Enterococcus and Escherichia coli are found in retail meat and in animals that are used as food. It also controls the resistance to Vibrio, Non-Zoonotic Enteric Pathogens, Shigella, E. coli 0157 and Typhoidal Salmonella in humans. NARMS acts as a one-heat solution promoting successful monitoring and study that plays an important role in combating resistance to antimicrobials. It has been operating for over 20 years, and the system will follow to serve as a manifesto addressing the growing antimicrobial resistance crisis.
Transatlantic Taskforce on Antimicrobial Resistance (TATFAR)
In 2009 CDC also set up TATFAR to address the urgent crisis of antibiotic resistance. In TATFAR countries like Canada, Norway, the United States, the European Union works in partnership to discuss the best operations to intensify the global and domestic efforts to overcome the crisis of antibiotic resistance [36].
Organization for Economic Co-Operation and Development (OECD)
The OECD is an international economic body. It acts as a discussion stage and gives affirmation to countries for the development of a productive and economic strategy to manage AMR, encourages the rational use of antibiotics and motivates research and development in the antibiotic sector. OECD includes about 34 member countries. As an average of around 10,000 to 40,000 USD was spent on treating a patient infected with a resistant bacteria[37], AMR has generated a notable impact on healthcare systems and financial statements in OECD.
Stemming the superbug flood, an OECD study released on November 7, 2018 included AMR ‘s prediction for 2050, how countries can fix it and also reduce tariffs. The report elaborates on the OECD inquiries, which consider three major measures, such as
Enhanced hand hygiene and environmental hygiene in the health care settings such as hospitals, Implementation of stewardship programmes
Creating awareness in the society by campaigns via mass media, use of quick diagnostic tests in order to postpone or avoid the prescription of antibiotics.
Intercession of the first two packages
These packages would minimize the cargo of AMR-induced diseases by 85%, 23% and 73% respectively 38.
Policies and Programms to Countries
Millions of people in the G20 countries are suffering from antimicrobial resistance and recognizing the importance of research and development in tackling the global AMR threat, the G20 has come up with a three-point perspective to revitalize the R&D sector. OECD has reported estimates of the existence of AMR for eight common bacteria in G20 countries, showing a rise from about 18% in 2010 to 22% in 2024, and will continue to rise to 28% by 2030 due to maximum antibiotic intake.
The statistics are focused on eight pathogens: E. coli (3rd generation cephalosporine and fluoroquinolone-resistant); K. pneumonia (carbapenem and immune to cephalosporins); P. aeruginosa (Carbapenem-resistance), E. faecalis (vancomycin-resistant), and E. faecium(vancomycin-resistant), S. aureus (resistant to methicillin), and S. pneumonia (Resistant to penicillin).
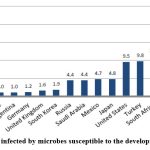 |
Figure 3: People infected by microbes susceptible to the development of resistanceClick here to view Figure |
The graph displays the following diseases: whooping cough, paratyphoid fever, typhoid fever, syphilis, lower respiratory tract infections, and meningitis. On June 29, 2017, a report titled “Tracking Antimicrobial Resistance – Sustainable R&D” was prepared in collaboration with the World Health Organization (WHO), the United Nations Food and Agriculture Organization (FAO), the World Organization for Animal Health (OIE), and the Organization for Economic Co-operation and Development (OECD).
Steering the basic research in academic institutions and small/medium scale industries by increasing the funding which projects G20’s Partnership plan as a knowledge capital for R and D. The support will be provided by WHO, OIE, OECD and FAO.
G20 would devote to support new guaranteeing antimicrobials in the Clinical Development phase aiming at the prioritized pathogens which needs immediate attention.
G20 would traverse the success of receiving financing mechanisms including pull mechanism that would pay for the novel antimicrobials which may lead to the disassociation of R &D funding from the trading income39.
Current Scenario
Recently, on 24 January 2019, WHO released a study on the “Top 10 Global Threats for 2019” and AMR was one of those that needed urgent notice40. An article published in the World Economic Forum on 27 March 2018 by Abdul Ghafur, Disease Consultant, reported that about 75,000 people die from AMR every year. In spite of incomplete and inaccurate data from all countries, a further study was released by the British government and predicted that by 2050 about 10 million people will die per year from AMR crisis. Because of its unregulated use, prescribing antibiotics even for common cold in many developed countries has led to AMR. To overcome these issues countries such as Finland have put in place strict antibiotic prescription regulations41. In 2017, the WHO categorized antibiotics into various categories on the basis of their site of action or their therapeutic and chemical properties. Every drug has been assigned an Anatomical Therapeutic Classification (ATC) code which is further classified as J, J01, J01C, J01CA and J01CA04 and has been given guidelines for the use of antibiotics in the treatment of 21 most severe infections42 but even these regulations do not help to overcome antibiotic resistance as many antibiotics can be obtained even without prescription.
Programms Executed by Government of India
A Red Line Campaign in India (2016)
India has introduced the red line program, which focuses on labelling prescription only antibiotics with a red line. The aim of this campaign is to discourage antibiotics counter-sales43.
Chennai Declaration (2012)
Indian Medical Associations adopted a collection of national guidelines, called the Chennai Declaration, to encourage antibiotic stewardship. It is a five-year plan to overcome antimicrobial resistance from an Indian perspective initiated at CIDSCON 2012. This was aimed at creating a National Policy to control and implement the emerging antimicrobial resistant by stakeholder representatives44.
Antimicrobial Stewardship Program
It is a multidisciplinary, hospital-based program which ICMR has developed guidelines. This is a co-ordinated operation involving optimal antimicrobial drug selection including dosage, length, and route of administration. Such guidelines should help the hospitals develop their own system of stewardship. The main aims of this program are to optimize safe and rational use of antibiotics with minimal adverse effects and improved effectiveness45.
National Programme for AMR Containment (2012-2017)
It was launched by the Ministry of Health with a network of 10 medical college laboratories across the country under the AMR surveillance programme. Spread now from eighteen states to 20 medical college laboratories46. Data collected by the National Program for AMR Containment was used to better understand the drug resistance, its immensity and to recognize the causes. A series of recommendations has been released by the National AMR Containment System including good prescribing writing practices, reserve antimicrobials, hypersensitivity, and antimicrobial warning.
National health policy addresses AMR as one of the main issues and urges the need to establish guidelines for antibiotic use, control over antibiotic use, deprive the use of antibiotics to promote development in domestic creatures, as well as pharmacovigilance plus prescription audit, antibiotic use in hospitals and society47.
National Action Plan on Antimicrobial Resistance NAP-AMR (2017- 2021)
AMR GAP-AMR Global Action Plan was announced at 68th World Health Assembly (WHA) in May 2015. Later WHA insisted that the GAP-AMR member states adopt the National Action Plan on AMR along with the GAP-AMR by March 2017. The Ministry of Health and Family Welfare has thus named three administrative structures, such as the Intersectional Coordinating Committee, the Technical Advisory Committee, and the core working group that established and drafted the National Plan of Action. It was reviewed under six strategic priorities, such as AMR.NAP-AMR, at the National Workshop on Developing the National Action Plan
Enhance consciousness and recognition of AMR through productive communication, education and training
Communication – to train all participants, includes policymakers, the broader population, and farmers
Education and training – to enhance professionals’ knowledge and behaviour.
Escalate surveillance to advance knowledge and proof
Advance laboratories – for evidence-based policymaking in the human, veterinary, agricultural, and environmental sectors.
Surveillance of AMR – for evidence-based policymaking in the human, veterinary, agricultural, and environmental sectors.
Understanding the need for prevention and control, thereby minimising the occurrence of infection.
Health maintenance – to minimise the risk of infection
Animal care – to prevent AMR and antimicrobial resistance from spreading through mammals and foodstuffs.
Public and community environment – to limit the spread of antimicrobial resistance and antimicrobials in the population and environment.
Rationalize the usage of antimicrobial agents in food, animals and health
Antimicrobial use regulations, access, and monitoring – to guarantee rational usage without jeopardising antimicrobial access
Antibiotic stewardship in healthcare – to improve antimicrobial usage in humans.
Livestock health and agriculture – to maximise antimicrobial usage in the animal and agricultural products
Encourage funding for AMR policies, research programmes and innovations
New drugs and investigations – to assure the availability of effective diagnostics and medications to treat infections.
Innovations – Possible altenative ways to infectious disease management are being developed.
Funding — to provide long-term resources for AMR control.
Reinforce India’s premiership on AMR
Collaborations with other countries – to secure India’s impacts on the global efforts to combat AMR.
National partnerships – to make it easier for vertical disease management initiatives and national stakeholders to work together.
Collaborations at the state level — to guarantee AMR action on the ground 48
Kerala Antimicrobial Resistance Strategic Action Plan (KARSAP)
Kerala is the first state to achieve a one-health manifesto involving health care and related sectors to restrain the antimicrobial resistance that is taking place. Government of Kerala launched a program to raise awareness among state stockholders of antimicrobial resistance. Under this initiative, the State Action Plan on Antimicrobial Resistance (AMR) will be implemented in accordance with the Global Action Plan on Antimicrobial Resistance (GAP-AMR) KARSAP and the National Action Plan on Antimicrobial Resistance (NAP-AMR).
The awareness programs insist on regulated antibiotic use, infection control and the need to follow institutional antibiotic policies. The Indian Medical Association (IMA) has done a fine job of uplifting policy development and guidance to students. Surveillance services are also managed by including hospitals and various private tertiary care clinics, including government teaching.
Infections of the bloodstream, infections of the skin and soft tissues, respiratory tract infections, urinary tract infections, and six other pathogens requiring immediate attention—Acinetobacter species, E. coli, Klebsiella species, Pseudomonas aeruginosa, Staphylococcus aureus, and Enterococcus species—are currently the focus of government medical colleges and general hospitals’ surveillance efforts and data collection. The Government Medical College, Trivandrum (GMCT) receives all of the gathered data and uses it to track the AMR drift over time.
As many prescription drugs are used in humans which ultimately affect the environment. Infection Prevention and control (IPC) has been involved in minimising the antimicrobial remains in the environment by distribution of Bio safety guidelines given by Central Poultry Development Organization which insists on the execution and encouragement of vaccines as an alternative to the antibiotic use. The use of antibiotics has also been regulated by the Drugs control department by obstructing over the counter sale, not of standard Quality drugs sale and abidance to the Red-line Campaign by Indian Government. In order to minimize the prescription of antibiotics all government colleges in Kerala have implemented the antimicrobial stewardship program (AMSP) and audits of the prescriptions are being carried out periodically49.
Madhya Pradesh State Action Plan for containment of Antimicrobial Resistance (MP-SPCAR)
The 2ndstate to have preparations for antimicrobial resistance is Madhya Pradesh. With this, MP became the 2ndstate to establish an action plan to control antimicrobial resistance (AMR) after Kerala.
According to the World Health Organization, AMR is a world-wide public health risk. Misappropriation use of antibiotic drugs in humans, livestock and aquaculture responsible for AMR. Furthermore, inadequate handling of waste from fields, healthcare services, manufacturers and households is contributing to a big crisis.
The use of antibiotics in the treatment of human illnesses is becoming unsustainable with increasing AMR. If timely action is not taken within limits, it is predicted that AMR will cause approximately 10 million deaths by 2050, resulting in significant worldwide economic losses. It will also harm nutritional wellbeing, livelihoods and delay the achievement of bearable progress goals.
The key goal of MP-SAPCAR is to approach AMR in a holistic way in the province. For eg, state-level surveillance of AMRs in all sectors like human health, animal agriculture, piscaries, the atmosphere and nourishment50.
Delhi Declaration on Antimicrobial Resistance – An Inter-ministerial Consensus
Delhi has developed an action plan to reduce antimicrobial resistance (AMR), making it the third state in India to do so after Madhya Pradesh and Kerala. AMR, a worldwide health hazard mostly brought on by insufficient use of antibiotics, might kill up to 10 million people by 2050, up from the current 70,000. “Resistance of a microorganism to an antimicrobial drug that was originally effective for the treatment of infections caused by it” is what the WHO defines as antimicrobial resistance (AMR).
The State Action Plan to Combat Antimicrobial Resistance (SAPCAR), which was introduced by the Delhi Government on January 3, 2020, aims to address AMR head-on. It emphasizes a “One Health” approach through multi-sectoral cooperation and six strategic priority areas51.
During the interministerial consultation on antimicrobial resistance, the Indian government committed to implementing a comprehensive and cooperative strategy for preventing and managing antimicrobial resistance (AMR).
Acknowledge that Antimicrobial Resistance is a serious matter; and its mainly due to inappropriate use in human, animal, food and agriculture sectors. Within AMR, resistance of antibiotics is the most urgent risks and to take an immediate attention52.
Programme by Government of Mauritius
Mauritius has made a major step towards the development of the National Action Plan on AMR using a OneHealth approach, guided by the OneHealth Committee, comprised of multiple stakeholders and particularly the quadripartite collaboration between the human, animal and plant health as well as the environment, essential for a holistic prevention, mitigation and response to anti-microbial resistance.
The Republic of Mauritius National Action Plan on Antimicrobial resistance 2017-2021was developed with 6 following strategic objectives [53,54]:
Engagement and education on AMR amongst all stakeholders;
Electronic surveillance of antimicrobial use and resistance in human, animal and environmental health;
Effective bio-security and infection prevention and control measures;
Evidence-based antimicrobial use in humans and animals;
Enforceable regulations to advance AMR prevention and containment; and
Equitable investment for National Action Plan Implementation.
Following which Mauritius has successfully developed its second national action plan on AMR 2024-2028, through a three-week robust workshop supported by the World Health Organization. The Ministry of Health and Wellness of Mauritius has shown great concern about the burden of AMR. A significant number of deaths in Mauritius can be attributed to hospital-acquired infections, many of which are caused by drug-resistant organisms. The global findings are also worrying with 1.27 million deaths caused by AMR while a further 4.95 million deaths are associated with AMR in 2019.
The 2024-2028 National Action Plan has been designed to provide a contextualized roadmap for confronting AMR in Mauritius. It outlines the key objectives, strategies, and interventions that will guide the country in tackling this important challenge. By strengthening surveillance and monitoring systems; improving infection prevention and control practices; promoting responsible antimicrobial use and prescription for humans and animals; and investing in research and innovation, Mauritius highly endeavors to preserve the efficacy of antimicrobials for generations to come.
Management and Response to AMR
An important factor in the emergence, spread, and transmission of AMR is the environment. As a result, the solution needs to be based on a One Health approach, which acknowledges the interdependence and indivisible nature of people, animals, plants, and the environment at all scales and including all sectors, stakeholders, and institutions. The environment plays a critical role in the solution, and prevention is at the heart of the action required to stop the formation of AMR.
AMR’s emergence and spread are significantly influenced by three economic sector value chains:
Production of chemicals and pharmaceuticals
Agriculture and food Aquaculture, food crops, and terrestrial animal production
Healthcare delivery hospitals, clinics, community health centres, and pharmacies that utilise a variety of chemicals and disinfectants.
AMR is also mostly caused by inadequate sanitation, wastewater, and associated waste effluent in systems that handle human and animal waste, such municipal wastewater.
Management options to address releases, effluent and waste, such as55
Pharmaceutical manufacturing
Making sure that waste and wastewater are adequately contained and treated. Integrate waste management into standard operating procedures that use a lifecycle approach to produce antimicrobials. Encourage manufacturers to use environmentally friendly payment and procurement methods.
Foodand Agriculture
To safeguard water supplies against contaminants, recalcitrant microbes, and antibiotic residue pollution, restrict usage and minimise outflows.
Implement infection prevention and control strategies.
Healthcare
Install wastewater treatment systems designed specifically for hospitals, particularly in areas lacking contemporary community wastewater treatment facilities. Utilise infection prevention and control initiatives and hospital stewardship to reduce the amount of AMR contaminants that contaminate the environment.
Municipals
Increase waste containment and optimize wastewater treatment and sludge management processes. Innovate and adapt wastewater treatment options, including technologies for differentresource
International Measures
The following are international measures that can be taken56:
Establishing and strengthening collaboration among international agencies, governments, nongovernmental organizations, and professional groups; Establishing surveillance networks for antimicrobial use and AMR globally; Building laboratory capacity for the detection and reporting of pathogens with AMR that have global health impacts; Establishing and strengthening international tracking systems for quick identification and mitigation of emerging pathogens; International monitoring to control counterfeit antimicrobials across the globe; Investing in research, new drug discovery, and vaccines.
Conclusion
Crisis of anti-microbial resistance can be resolved by avoiding the overuse and abuse of antibiotics, continuous monitoring by surveillance systems, providing information, rationalizing antibiotic use and creating new antibiotics. AMR can be tackled internationally by establishing strict guidelines and joint efforts and collective government, medical associations and hospitals. Although as of November 2023, 178 countries had developed AMR national action plans aligned with Global Action Plan on AMR. To ensure sustained progress, countries need to establish a functioning multisectoral AMR governance mechanism, prioritize activities, develop a costed operational plan, mobilize resources (both domestic and external), and effectively implement their plan. Monitoring mechanisms are needed to track progress, identify challenges and report periodically. To globally track the progress in AMR national action plan implementation, countries have committed to completing the multisectoral annual Tracking AMR Country Self-Assessment Survey (TrACSS) [57-58]. This is the only path ahead in combating antimicrobial resistance.
Acknowledgement
The authors acknowledge JSS College of Pharmacy, Ooty – JSS Academy of Higher Education & Research, Mysore for providing adequate facilities to carry out original research related to antimicrobial resistance in association with Government Medical College and Hospital, Ooty
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Authors’ Contribution
V.K. (Vatsa Kapadia); R.B (Rihana Begum); P.K (Piyush Kumar): Conceptualization, Data collection, Writing original draft.
A.W. (Ashish Wadhwani); Sivasankara Ponnusankar (S.P.): Visualization, Supervision, Project Administration and funding acquisition for original research project.
M.G (Medha Gujadhur): Data collection
P.M. (Praveen Mohadeb): Visualization and Proof reading the manuscript
References
- Khan AA, Manzoor KN, Sultan A, et al. Pulling the Brakes on Fast and Furious Multiple Drug-Resistant (MDR) Bacteria. Int. J Mol Sci. 2021; 22(2):859. doi:10.3390/ijms22020859
CrossRef - Walker B, Barrett S, Polasky S, Galaz V, Folke C, Engström G, Ackerman F, Arrow K, Carpenter S, Chopra K, Daily G, Ehrlich P, Hughes T, Kautsky N, Levin S, Mäler K-G, Shogren J, Vincent J, Xepapadeas T, de Zeeuw A. Environment. Looming global-scale failures and missing institutions. Science. 2009; 325 (5946):1345-1346. doi:10.1126/science.1175325
CrossRef - Klevens RM, Morrison MA, Nadle J, Petit S, Gershman K, Ray S, Harrison LH, Lynfield R, Dumyati G, Townes JM, Craig AS, Zell ER, Fosheim GE, McDougal LK, Carey RB, Fridkin SK, Active Bacterial Core surveillance (ABCs) MRSA Investigators. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298(15):1763-1771. doi:10.1001/jama.298.15.1763
CrossRef - Klevens RM, Edwards JR, Richards Jr CL, Horan TC, Gaynes RP, Pollock DA, Cardo DM. Estimating health care-associated infections and deaths in US hospitals, 2002. Public health reports. 2007 Mar;122(2):160-6. Accessed February 9, 2021.
CrossRef - Eber MR, Laxminarayan R, Perencevich EN, Malani A. Clinical and economic outcomes attributable to health care-associated sepsis and pneumonia. Arch Intern Med. 2010;170(4):347-353. doi:10.1001/archinternmed.2009.509
CrossRef - Vincent J-L, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, EPIC II Group of Investigators. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323-2329. doi:10.1001/jama.2009.1754
CrossRef - Roberts RR, Hota B, Ahmad I, Scott II RD, Foster SD, Abbasi F, Schabowski S, Kampe LM, Ciavarella GG, Supino M, Naples J, Cordell R, Levy SB, Weinstein RA. Hospital and Societal Costs of Antimicrobial‐Resistant Infections in a Chicago Teaching Hospital: Implications for Antibiotic Stewardship. Clin Infect Dis. 2009;49(8):1175-1184. doi:10.1086/605630
CrossRef - Mauldin PD, Salgado CD, Hansen IS, Durup DT, Bosso JA. Attributable hospital cost and length of stay associated with health care-associated infections caused by antibiotic-resistant gram-negative bacteria. Antimicrob Agents Chemother. 2010;54(1):109-115. doi:10.1128/AAC.01041-09
CrossRef - Filice GA, Nyman JA, Lexau C, Lees CH, Bockstedt LA, Como-Sabetti K, Lesher LJ, Lynfield R. Excess costs and utilization associated with methicillin resistance for patients with Staphylococcus aureus infection. Infect Control Hosp Epidemiol. 2010;31(4):365-373. doi:10.1086/651094
CrossRef - Ocampo-Ibáñez ID, Liscano Y, Rivera-Sánchez SP, et al. A Novel Cecropin D-Derived Short Cationic Antimicrobial Peptide Exhibits Antibacterial Activity Against Wild-Type and Multidrug-Resistant Strains of Klebsiella pneumoniae and Pseudomonas aeruginosa. Evol Bioinform Online. 2020; 16:1176934320936266. doi:10.1177/1176934320936266
CrossRef - Tiwari R, Dhama K. Antibiotic Resistance: A Frightening Health Dilemma. American J Pharmacol and Toxicol. 2014;9(3):174-176. doi:10.3844/ajptsp.2014.174.176
CrossRef - Gould IM, Bal AM. New antibiotic agents in the pipeline and how they can help overcome microbial resistance. Virulence. 2013;4(2):185-191. doi:10.4161/viru.22507
CrossRef - Centers for Disease Control and Prevention (U.S.). Antibiotic Resistance Threats in the United States, 2019. Centers for Disease Control and Prevention (U.S.); 2019. doi:10.15620/cdc:82532
CrossRef - Reygaert WC. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018;4(3):482-501. doi:10.3934/microbiol.2018.3.482
CrossRef - Griffith M, Postelnick M, Scheetz M. Antimicrobial stewardship programs: methods of operation and suggested outcomes. Expert Rev Anti Infect Ther. 2012;10(1):63-73. doi:10.1586/eri.11.153
CrossRef - Yu VL. Guidelines for hospital-acquired pneumonia and health-care-associated pneumonia: a vulnerability, a pitfall, and a fatal flaw. The Lancet Infectious Diseases. 2011;11(3):248-252. doi:10.1016/S1473-3099(11)70005-6
CrossRef - Stockwell VO, Duffy B. Use of antibiotics in plant agriculture. Rev Sci Tech. 2012;31(1):199-210. doi:10.20506/rst.31.1.2104
CrossRef - Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309-318 doi:10.1179/2047773215Y.0000000030
CrossRef - Bouki C, Venieri D, Diamadopoulos E. Detection and fate of antibiotic resistant bacteria in wastewater treatment plants: a review. Ecotoxicol Environ Saf. 2013; 91:1-9. doi: 10.1016/j.ecoenv.2013.01.016
CrossRef - Infectious Diseases Society of America (IDSA), Spellberg B, Blaser M, Guidos RJ, Boucher HW, Bradley JS, Eisenstein BI, Gerding D, Lynfield R, Reller LB, Rex J, Schwartz D, Septimus E, Tenover FC, Gilbert DN. Combating antimicrobial resistance: policy recommendations to save lives. Clin Infect Dis. 2011;52 Suppl 5: S397-428. doi:10.1093/cid/cir153
CrossRef - Conly JM. Antimicrobial resistance – Judicious use is the key. Can J Infect Dis Med Microbiol. 2004;15(5):249-251.
CrossRef - Doron S, Davidson LE. Antimicrobial stewardship. Mayo Clin Proc. 2011;86(11):1113-1123. doi:10.4065/mcp.2011.0358
CrossRef - MacDougall C, Polk RE. Antimicrobial stewardship programs in health care systems. Clin Microbiol Rev. 2005;18(4):638-656. doi:10.1128/CMR.18.4.638-656.2005
CrossRef - Majumder MAA, Rahman S, Cohall D, et al. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infect Drug Resist. 2020;13:4713-4738. doi:10.2147/IDR.S290835
CrossRef - Uchil RR, Kohli GS, Katekhaye VM, Swami OC. Strategies to Combat Antimicrobial Resistance. J Clin Diagn Res. 2014;8(7):ME01-ME04. doi:10.7860/JCDR/2014/8925.4529
CrossRef - WHO | The WHO policy package to combat antimicrobial resistance. WHO. Accessed February 9, 2021. https://www.who.int/bulletin/volumes/89/5/11-088435/en/
- Antimicrobial resistance – SEA/RC68/R3. Accessed February 9, 2021. https://apps.who.int/iris/handle/10665/190978?show=full
- Choy CY, Hsu LY. World Antibiotic Awareness Week. Ann Acad Med Singap. 2017;46(11):413-414.
CrossRef - GLASS | Global antimicrobial resistance surveillance system (GLASS) report. Accessed February 10, 2021. https://www.who.int/glass/resources/publications/early-implementation-report/en/
CrossRef - V. Piddock LJ. The global antibiotic research and development partnership (GARDP): researching and developing new antibiotics to meet global public health needs. MedChemComm. 2019;10(8):1227-1230. doi:10.1039/C9MD90010A
- WHO | UN Interagency Coordination Group (IACG) on Antimicrobial Resistance. WHO. Accessed February 9, 2021. http://www.who.int/antimicrobial-resistance/interagency-coordination-group/en/
- Organization WH. Global antimicrobial resistance surveillance system (GLASS): technical meeting on the early implementation phase: 22-23 October 2015: WHO Regional Office for Europe Copenhagen, Denmark: meeting report. Published online 2016. Accessed February 10, 2021. https://apps.who.int/iris/handle/10665/204117
- CDC. What CDC is Doing: Antibiotic Resistance (AR) Solutions Initiative. Centers for Disease Control and Prevention. Published November 6, 2020. Accessed February 9, 2021. https://www.cdc.gov/drugresistance/solutions-initiative/index.html
- National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS) | NARMS | CDC. Published October 2, 2020. Accessed February 9, 2021. https://www.cdc.gov/narms/index.html
- Karp BE, Tate H, Plumblee JR, Dessai U, Whichard JM, Thacker EL, Hale KR, Wilson W, Friedman CR, Griffin PM, McDermott PF. National Antimicrobial Resistance Monitoring System: Two Decades of Advancing Public Health Through Integrated Surveillance of Antimicrobial Resistance. Foodborne Pathog Dis. 2017;14(10):545-557. doi:10.1089/fpd.2017.2283
CrossRef - Centers for Disease Control and Prevention (CDC). Transatlantic Taskforce on Antimicrobial Resistance Recommendations for Future Collaboration between the US and EU. Atlanta. 2014;500(2011):1-45.
- Hofer U. The cost of antimicrobial resistance. Nat Rev Microbiol. 2019;17(1):3. doi:10.1038/s41579-018-0125-x
CrossRef - Stemming the Superbug Tide: Just A Few Dollars More | en | OECD. Accessed February 9, 2021. https://www.oecd.org/health/stemming-the-superbug-tide-9789264307599-en.htm
- Tackling antimicrobial resistance, http://www.oecd.org/g20/summits/hamburg/Tackling-Antimicrobial-Resistance-Ensuring-Sustainable-RD.pdf, Accessed September 10, 2021
- Ten threats to global health in 2019. Accessed February 9, 2021. https://www.who.int/vietnam/news/ feature-stories/detail/ten-threats-to-global-health-in-2019
- Weltwirtschaftsforum, Zurich Insurance Group. Global Risks 2019: Insight Report.; 2019. Accessed February 10, 2021. http://www3.weforum.org/docs/ WEF_Global_Risks_Report_2019.pdf
- Srivastava R. India lauded for Red Line Campaign on antibiotics. The Hindu. https://www.thehindu.com/news/national/india-lauded-for-red-line-campaign-on-antibiotics/article8622474.ece. Published May 20, 2016. Accessed February 10, 2021.
- Ghafur A, Mathai D, Muruganathan A, Jayalal JA, Kant R, Chaudhary D, Prabhash K, Abraham OC, Gopalakrishnan R, Ramasubramanian V, Shah SN, Pardeshi R, Huilgol A, Kapil A, Gill JPS, Singh S, Rissam HS, Todi S, Hegde BM, Parikh P. The Chennai declaration: A roadmap to tackle the challenge of antimicrobial resistance. Indian Journal of Cancer. 2013;50(1):71. doi:10.4103/0019-509X.104065
CrossRef - National Treatment Guidelines for Antimicrobial Use in Infectious Diseases Available at: https://ncdc.gov.in/WriteReadData/l892s/File622.pdf, Accessed October 3, 2021
- National Programme on AMR Containment: National Centre for Disease Control (NCDC). Accessed February 10, 2021. https://ncdc.gov.in/index1.php?lang=1&level=2&sublinkid=384&lid=344
- National Health Policy. Accessed February 10, 2021. https://cdsco.gov.in/opencms/opencms/en/ consumer/National-Health-Policy/
- National action plan on AMR (NAP-AMR): National Centre for Disease Control (NCDC). Accessed February 10, 2021. https://www.ncdc.gov.in/index1.php?lang=1&level=2&sublinkid=389&lid=347
- http://iamrsn.icmr.org.in/index.php/amsp/amsp-guidelines, Accessed October 10, 2021
- Kerala Antimicrobial Resistance Strategic Action Plan (KARSAP). Government of Kerala, October 2018 https://ncdc.mohfw.gov.in/wp-content/uploads/2024/03/ 35158354141579866436.pdf
- Madhya Pradesh second state to have plan for antimicrobial resistance. Accessed October 25, 2020. https://www.downtoearth.org.in/blog/health/madhya-pradesh-second-state-to-have-plan-for-antimicrobial-resistance-65954
- Pioneer T. Delhi 3rd in country to develop action plan to tackle AMR menace. The Pioneer. Accessed October 25, 2020. https://www.dailypioneer.com/2020/india/delhi-3rd-in-country-to-develop-action-plan-to-tackle-amr-menace.html
- Delhi Declaration of Antimicrobial resistance https://ncdc.gov.in/WriteReadData/linkimages/ AMR/File670.pdf, Accessed November 19, 2021
- Republic of Mauritius National Action Plan on Antimicrobial Resistance; 2017-2021 Ministry of Health and Quality of Life. Published on 17th April 2017
- Antimicrobial Consumption Monitoring in Mauritius. 23rd January 2018. https://www.afro.who.int/news/antimicrobial-consumption-monitoring-mauritius
- UN environment programme. Antimicrobial resistance: a global threat. https://www.unep.org/ topics/chemicals-and-pollution-action/pollution-and-health/antimicrobial-resistance-global-threat
- Salam, M.A.; Al-Amin, M.Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare 2023, 11, 1946. https://doi.org/10.3390/ healthcare11131946
CrossRef - WHO Antimicrobial resistance News 21 November 2023. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
- Antimicrobial Resistance Collaborators. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet; 399(10325): P629-655. DOI: https://doi.org/10.1016/S0140-6736(21)02724-0
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



