

How to Cite | Publication History | PlumX Article Matrix
Unexplained Pain Due to the Retained Surgical Item in the Abdominal Cavity: A Rare Presentation
Mohammad Sadegh Sanie1, Lohrasb Taheri2, Mohamed Amin Ghobadifar3* and Navid Kalani4
1Department of Anaesthesiology, Jahrom University of Medical Sciences, Jahrom, Iran.
2Department of General Surgery, Jahrom University of Medical Sciences, Jahrom, Iran.
3Zoonoses Research Center, Jahrom University of Medical Sciences, Jahrom, Iran.
4Department of Student Research Committee, Jahrom University of Medical Sciences, Jahrom, Iran.
DOI : http://dx.doi.org/10.13005/bbra/2176

ABSTRACT: Retained surgical items (RSI) is a problem of surgical patient safety. RSIs after surgical procedures in the abdomen are critical causes of intraperitoneal infections. Unexplained pain due to the RSIs after a surgery is a rare presentation. There are few publications in the worldwide literature described manifestations associated with RSIs. In this article, we report a rare case presented with unexplained and persistent abdominal pain associated with a hemovac cap forgotten in the abdominal cavity a few months ago. A 52-year-old female presented to our clinic with abdominal pain, constipation, nausea, vomiting, and pyrexia of unknown origin. She had a history of oophorectomy and total abdominal hysterectomy to decrease the risk of ovarian cancer. Clinical examination revealed painful and distended abdominal wall with fever. Abdominal X-ray analysis showed extensively air-filled small and large bowels. A laparotomy was performed, and interestingly, a retained hemovac cap was found which was densely adherent to the surrounding bowel. This case report shows that unexplained and persistent abdominal pain can represent due to RSI after abdominal surgical procedures.
KEYWORDS: Abdominal abscess; Abdominal cavity; Abdominal pain; Foreign bodies; Hysterectomy; Surgery
Download this article as:| Copy the following to cite this article: Sanie M. S, Taheri L, Ghobadifar M. A, Kalani N. Unexplained Pain Due to the Retained Surgical Item in the Abdominal Cavity: A Rare Presentation. Biosci Biotech Res Asia 2015;12(spl.edn.2) |
| Copy the following to cite this URL: Sanie M. S, Taheri L, Ghobadifar M. A, Kalani N. Unexplained Pain Due to the Retained Surgical Item in the Abdominal Cavity: A Rare Presentation. Biosci Biotech Res Asia 2015;12(spl.edn.2). Available from:https://www.biotech-asia.org/?p=12801 |
Introduction
RSI may be detected acutely during the immediate post-operative period [1]. It may produce serious immediate or early-term post-operative complications, or stay dormant for months to years [2]. When incorrectly diagnosed or not immediately recognized, RSI can cause significant harm to the patients, including surgical procedures, additional diagnostic tests, various complications, and even mortality [3]. The pelvic and abdominal cavities are the most common sites of RSIs. It accounts for about one-half of all RSIs [4]. The most commonly encountered symptoms related to the abdominal RSI are intestinal obstruction and nonspecific abdominal pain [5]. Due to ethical and legal reasons, only a few reports in the worldwide literature described manifestations associated with RSI after abdominal surgical process. Here, we described such a case involving a 52-year-old female with a history of total abdominal hysterectomy, presented with unexplained and persistent abdominal pain and pyrexia with unknown origin. Subsequently, a retained hemovac cap which was densely adherent to the surrounding bowel revealed after laparotomy. For publication of this case-report and accompanying images, written informed consent was obtained from the patient.
Case presentation
A 52-year-old female presented to our surgical outpatient clinic with abdominal pain, anorexia, abdominal distention, nausea, vomiting, and pyrexia. The patient suffered from generalized unexplained and persistent abdominal pain which was progressive, and she had a low grade pyrexia for at least 3 months. Her fever was intermittent and most frequent in the early morning and night. She had a past medical history of oophorectomy and total abdominal hysterectomy to decrease the risk of ovarian cancer 4 months ago. Unexplained abdominal pain ensued following her past surgery. Physical examination revealed generalized tenderness from the epigastric to the pelvic area. Blood results presented high C-reactive protein (>200), high erythrocyte sedimentation rate (>50), normochromic normocytic anemia, leukocytosis, and mildly increased alkaline phosphatase levels. No obvious source of infection which would cause of the fever was found. Repeated blood cultures yielded no bacterial growth. No improvement of the fever was seen after treating her with broad spectrum antibiotics.
X-ray analysis and ultrasonography (USG) of the abdominal cavity were carried out, and both showed deviation from normal conditions but a foreign body retained in the abdomen was not noticed. Abdominal X-ray analysis showed extensively air-filled small and large bowels. USG analysis indicated moderate fatty liver infiltration. Due to the lack of visual tags, the foreign body retained in the abdominal cavity was not noticed. After the patient had been consented for surgery, surprisingly, a retained hemovaccap (Fig. 1) at the bottom of cavity which was densely adherent to the surrounding bowel with an abscess formation all around it revealed and retrieved immediately. Also, numbers of adhesions were partially separated in the abdominal cavity. No mass or tumor was found in liver, spleen and pelvic area during the laparotomy. Two liters of abscess was aspirated and subsequently sent for cytological examination which revealed no classes of tumor. Furthermore, a 1×2 cm excision biopsy of surrounding tissue adherent to the retained foreign body sent for histopathological examination and immunohistochemical analysis which revealed no obvious documentation of tumor cells. An uneventful postoperative recovery was reported for the patient, and the pyrexia completely resolved following the surgery.
Two months following the retained hemovac cap retrieval from the abdominal cavity, the patient was re-admitted with acute abdominal pain. On the X-ray analysis, she was found to have centrally located multiple dilated loops of gas filled bowel. Following to her acute abdomen and mechanical obstruction, the patient was referred to the surgical department, and the abdominal fossa was re-opened. Multiple adhesion bands were seen in the lower parts of the intestinal lumen, subsequently, adhesions were partially separated in the abdominal cavity. Postoperative recovery was uneventful. The patient was followed-up for more than 5 months, and she showed excellent improvement in abdominal pain without any complications. Therefore, the patient was able to return to her daily life.
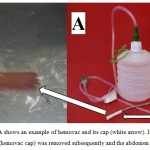 |
Figure 1: Part A shows an example of hemovac and its cap (white arrow). In part B the object (hemovac cap) was removed subsequently and the abdomen closed.
|
Discussion
The incidence of RSI after abdominal surgery is very low and purposely underreported [5]. RSI specially refers to surgical materials such as supplies, equipment, and tools that are used by surgical providers, but may accidently be left in patients’ body. Amorphous structure, and small sized surgical items are the most frequently encountered RSI after abdominal surgery [6].The presence of RSI has been demonstrated to be associated independently with emergency surgery, Contributing factors can involve lack of surgical sponge/instrument count, involvement of multiple surgical teams’, unplanned change of plan during surgical procedure, longer duration of operation, incorrect surgical count, and performing more than one procedure in the course of the same operation [7]. Generally, the risk of RSI is higher in emergency surgical procedures compared to elective surgeries. Furthermore, patients who undergo surgical procedures without instrument count are at higher risk for RSI [8]. The hemovac cap retained in the abdominal cavity in the patient of the present study is a small sized surgical items, but her past surgical history was not an emergency surgical procedure. Inaccuracy of the surgeon and the operating room staff may be associated risk factor for RSI in the patient of the current study.
Prevention of RSI requires constant surveillance of the surgeon and operation room team to inhibit this potential threat of surgical safety. The surgeon must enumerate for an incorrect instrument count by sufficient examination of the operative field when in doubt. Re-counting instrument as well as precise searching of the operative field may prevent RSI. Abdominal cavity inspection prior to closure in all patients should be done in routine with an especial attention to the groups of patients who are at high risk for RSI [9]. Another way to reduce the risk of RSI is clear verbal communication between surgeon(s) and the surgical team in regard to the precise location and number of instrument or other surgical object. In addition, it is critical to correlate any abnormal or nonspecific findings detected on imaging tests carried out to rule out RSI in the patient with the past surgical history.
Clinical manifestations of abdominal RSIs are caused by multifactorial interactions among following elements: (I) presence of infection; (II) the nature of the retained surgical items; (III) precise anatomic location of the retained surgical items; and (IV) various patient factors [10]. Impermanent presentation of gastrointestinal complications of RSI varies widely (i.e. they may present immediately or their manifestations may be delayed for months to years). Metallic and plastic instruments usually cause immediate or acute clinical symptoms during immediate postoperative period, in comparison surgical sponge retention may cause frequently a chronic progression of manifestations over months to years [11]. Acute manifestation is usually associated with intestinal obstruction, pain, abscess, sepsis, and granuloma formation. While, chronically abdominal RSI may present as a mass or progressive intestinal obstruction associated with subsequent adhesion formation and encapsulation of RSI. Various types of fistulae has been also reported as the clinical presentation of RSIs [12]. The patient in the current study suffered from pain, intestinal obstruction due to the adhesion bands formation, and abscess formation which all belongs to clinical manifestation of RSI.
Nonspecific abdominal symptoms may be the result of exudative reaction of the RSI. Unexplained intermittent or persistent abdominal pain and persistent or recurrent postoperative ileus may occur several months after laparotomy when surgical item is retained in the abdominal cavity [13]. Patients with RSI may acutely present with the finding of intraperitoneal abscess formation with associated symptoms and signs of sepsis. Hence, patients with intraperitoneal abscess due to RSI are most frequently presented with abdominal pain and fever. Clinical management consists of retrieval of the RSI, abscess drainage, and abdominal washout [14]. Inflammatory reaction surrounding a RSI may be the reason for intestinal obstruction. Bowel obstruction associated with RSI may acutely manifest as a simple postoperative intestinal obstruction or may be associated with abdominal mass in a chronic setting [15]. Management includes of standard therapy for intestinal obstruction and removal of RSI. After operative removal of RSI, obstructive manifestations are relieved.
There are different techniques to identify RSI in the abdominal or pelvic cavity, such as radiopaque marking. However, radiopaque markers are not routinely used because they may get attached to the bone or become degenerated over the period of the time in which they may get folded, distorted or twisted [16]. X-ray analysis can be used for demonstrating of RSI. Unfortunately, it is very hard to discover missing needles, caps, and such. A high resolution of X-ray does not guarantee that the missing items are not inside the patient [17]. USG diagnoses the nature of the mass (solid or liquid) in three dimensions. Nevertheless, USG is not a good method in the presence of gas or fat in the abdomen. X-ray analysis and USG were performed for the patient in the present study, but foreign body retained in the abdominal cavity was not noticed. The possible reasons behind this no visibility of RSI include the type of RSI (cap) and presence of gas and fat in the abdominal cavity.
Abdominal pain completely resolved following the second time of laparotomy in the patient of the current study. This case report shows that unexplained and persistent abdominal pain can represent due to the RSI after abdominal surgical procedures. In this regard, physicians must be aware of RSI while considering differential diagnosis for patients with history of surgery in abdominal cavity that are presented with unexplained and persistent abdominal pain and symptoms associated with systemic inflammatory response.
References
- Kaiser CW, Friedman S, Spurling KP, Slowick T, Kaiser HA. The retained surgical sponge. Ann Surg. 1996;224(1):79-84.
- Hyslop JW, Maull KI. Natural history of the retained surgical sponge. South Med J. 1982;75(6):657-60.
- Yildirim S, Tarim A, Nursal TZ, Yildirim T, Caliskan K, Torer N, et al. Retained surgical sponge (gossypiboma) after intraabdominal or retroperitoneal surgery: 14 cases treated at a single center. Langenbecks Arch Surg. 2006;391(4):390-5.
- Lincourt AE, Harrell A, Cristiano J, Sechrist C, Kercher K, Heniford BT. Retained foreign bodies after surgery. J Surg Res. 2007;138(2):170-4.
- Berkowitz S, Marshall H, Charles A. Retained intra-abdominal surgical instruments: time to use nascent technology? Am Surg. 2007;73(11):1083-5.
- Possover M. Images in clinical medicine. Gossypiboma in the pouch of Douglas. N Engl J Med. 2008;359(8):e9.
- National Environmental Policy Act of 1969, (May 15, 1969, 1994).
- Egorova NN, Moskowitz A, Gelijns A, Weinberg A, Curty J, Rabin-Fastman B, et al. Managing the prevention of retained surgical instruments: what is the value of counting? Ann Surg. 2008;247(1):13-8.
- Sharma G, Bigelow J. Retained foreign bodies: a serious threat in the Indian operation room. Ann Med Health Sci Res. 2014;4(1):30-7.
- Stawicki SP, Evans DC, Cipolla J, Seamon MJ, Lukaszczyk JJ, Prosciak MP, et al. Retained surgical foreign bodies: a comprehensive review of risks and preventive strategies. Scand J Surg. 2009;98(1):8-17.
- Schonleben K, Strobel A, Schonleben F, Hoffmann A. [Retained foreign bodies from the surgical point of view]. Chirurg. 2007;78(1):7-12.
- Wang CF, Cipolla J, Seamon MJ, Lindsey DE, Stawicki SP. Gastrointestinal complications related to retained surgical foreign bodies (RSFB): A concise review. OPUS. 2007;12:11-8.
- Rumstadt B, Roshanaei N, Schilling D. [Gossypiboma – the retained surgical towel]. Dtsch Med Wochenschr. 2008;133(33):1673-6.
- Khan HS, Malik AA, Ali S, Naeem A. Gossypiboma as a cause of intestinal obstruction. J Coll Physicians Surg Pak. 2014;24 Suppl 3:S188-9.
- Colak T, Olmez T, Turkmenoglu O, Dag A. Small Bowel Perforation due to Gossypiboma Caused Acute Abdomen. Case Rep Surg. 2013;2013:219354.
- Takigami I, Itoh Y, Itokazu M, Shimizu K. Radio-opaque marker of a surgical sponge appearing as an intra-articular foreign body after total hip arthroplasty. Arch Orthop Trauma Surg. 2008;128(10):1167-8.
- Cheng TC, Chou AS, Jeng CM, Chang PY, Lee CC. Computed tomography findings of gossypiboma. J Chin Med Assoc. 2007;70(12):565-9.

This work is licensed under a Creative Commons Attribution 4.0 International License.



