

How to Cite | Publication History | PlumX Article Matrix
Fatemeh Ghavi1, Leili Mosalanejad2, Masomeh Golestan3 and Mina Taheri4
1Assistant professor, Midwifery Department, Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran 2Assistant professor, Mental Health Department, Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran 3Research and Clinical Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran 4Lecturer in Midwifery,Department of Midwifery ,College of Nursing and Midwifery Shiraz,University of Medical Science,Shiraz;Iran
DOI : http://dx.doi.org/10.13005/bbra/1864

ABSTRACT: The recognition of the distressing character of infertility diagnosis and treatment has led to the development of many researches in medical psychology and mental health domain .This article aimed to investigate holistic stress from infertility by gender difference. This is a cross-sectional descriptive study on 369 infertile couples (175 male and 194 women) who referred to Yazd infertility center. These participants were selected by purposive sampling method. Data were collected by using demographic characteristics’ questionnaire (researcher-made questionnaire), DASS test( depression- anxiety- stress ) , Courdon stress test( health stress- personality stress and life stress ) and perceived stress test ( positive and negative perceived stress) . Mean score of depression, anxiety and stress in women was higher than men. Negative perceived stress, personality stress and life stress in women was higher than men, but positive stress conceived and health stress in men was higher than women. The results show that infertility has a significant impact on couples over time. Mental health professionals can educate couples regarding the effectiveness of coping strategies as well as stress management techniques while experiencing the stress of infertility.
KEYWORDS: Stress; Infertility; Sex; Depression; Anxiety
Download this article as:| Copy the following to cite this article: Ghavi F, Mosalanejad L, Golestan M, Taheri M. A Holistic Approach for Comparing Stress by Gender Difference in Couple Who Received Assisted Reproductive Treatment. Biosci Biotech Res Asia 2015;12(3) |
| Copy the following to cite this URL: Ghavi F, Mosalanejad L, Golestan M, Taheri M. A Holistic Approach for Comparing Stress by Gender Difference in Couple Who Received Assisted Reproductive Treatment. Biosci Biotech Res Asia 2015;12(3). Available from: https://www.biotech-asia.org/?p=2227 |
Introduction
Infertility is a biopsychosocial phenomenon in which mental, physiological, environmental and interpersonal variables interact with each other. Therefore, infertility cannot be solely considered as a physical disorder (1). The World Health Organization (WHO), considers infertility as a global public health issue (2) inflicting 80-168 million individuals worldwide (3).
In a epidemiological study investigating the causes of infertility in patients referred to Royan institute, 50.5%, 28.6%, and 11.6% of the participants had the male factor infertility, female factor infertility, or both, respectively. Moreover, 9.3% of the infertile participants had infertility with an unknown etiology (4). In general, most studies hae indicated that the female and male factors each have a share of about one third of infertilities; while 20% of the remaining one third has unknown etiology and the rest is related to both couples (5).
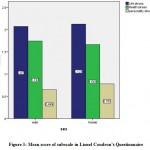 |
Figure 1: Mean score of subscale in Lionel Coudron’s Questionnaire |
In Iran, the prevalence of lifetime primary infertility was 24.9% during 2004-2005, comprising one fourth of Iranian couples (6). Since, conception and having children is considered as a personal, social, and cultural value, infertile individuals strive to diagnose and treat the cause of their infertility. In the meantime, they experience and bear many mental tensions because of the biopsychosocial burdens of infertility treatment. In fact, infertility is accompanied by increased psychological stresses (7).
Dealing with infertility immensely affects the lives of men and women and puts them at risk of emotional problems as well as physical, financial, and mental challenges related to assisted reproductive methods. Such challenges pave the way for depression during the late 20s and 30s in many individuals (8). Johnson and colleagues reported that 50% of women and 15% of men consider infertility as their most stressful life experience (9).Another study also showed a relationship between anxiety and stress and male and female infertility (10).
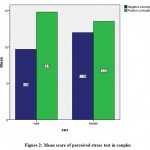 |
Figure 2: Mean score of perceived stress test in couples |
Considering the influential cultural, economical and educational differences of infertile men, some studies have shown psychological problems in this group (11). Infertile men have less stress and higher mental health compared with infertile women. Studies indicate that disorders such as depression are more prevalent in women (12). Women specifically suffer from mental stresses of infertility and are more anxious and depressed compared to their spouse and have lower self-esteem (13).
Ignoring the psychological complications of infertile couples leads to a vicious cycle that would in turn reduce the possibility of treatment. Moreover, with respect to the effects of infertility on marital and social relationships, informative and mental support programs in Iran have not been successful. Therefore, understanding the psychological problems of infertile men and women is necessary for devising related psychological interventions.
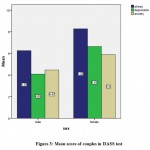 |
Figure 3: Mean score of couples in DASS test |
On the other hand, most studies on stress and psychological reactions of infertile men and women have considered confounding factors such as cause of infertility, duration of infertility, hope to being treated, family configuration, and number of treatment cycles. However, the results of these studies differed based on ethnicity and study conditions. Moreover, these studies were not done in Iran and cannot be generalized to the Iranian population. Therefore, we aimed to compare the psychological stresses of infertile men and women in an Iranian sample.
Patients and Methods
In this cross-sectional study, we assessed the stresses of infertile men and women and their relation to demographic factors in 398 individuals receiving assisted reproductive services in the Infertility Center of Yazd, Iran. The study population consisted of all individuals who referred to this center during 2013. Considering an infertility prevalence of 5-15%, the sample size was calculated to be 400 (200 men and 200 women). The proposal of the study was confirmed by the Ethics Committee of Jahrom University of Medical Sciences. Individuals participated in the study at their own free will and are assured that they could leave the study at any desirable point.
(Here, it is better to mention the exclusion and inclusion criteria of the study completely.)
Data were collected using four questionnaires: a demographic data questionnaire, the depression anxiety stress scale short form (DASS-21) and the perceived stress scale, and the Courdon stress test. The DASS-21 is a 21-item instrument designed to measure the 3 negative affective states of depression, anxiety, and stress. The depression scale evaluates dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest or involvement, anhedonia, and inertia. The anxiety scale measures autonomic arousal, situational anxiety, and subjective experience of anxious affect. The stress scale assessed difficulty relaxing, nervous arousal, and being easily upset or agitated, irritable, or over-reactive and impatient (14). in this research we used the cutoff scores suggested by Lovibond and Lovibond (15-16). The psychometric properties of the DASS have been extensively evaluated, and there is evidence for the convergent and discriminative validity of data obtained with this instrument (17-18).
The Perceived Stress Scale (PSS-14) is a 14-item self-report questionnaire that measures persons’ evaluation of the stressfulness situations in the past month of their lives. Respondents report the prevalence of an item within the last month on a 5-point scale, ranging from never to very often. Responses are measured on a five-point scale (0=never, 1=almost never, 2=sometimes, 3=fairly often, 4=very often). Cohen and Williamson (1988) have established its reliability and validity (r=0.85) and internal reliability (r=0.60) (19).
To evaluate general stress in different situations, the Courdon stress test was used. It is a standardized questionnaire with suitable reliability and validity as shown in previous studies. In repeated use of this questionnaire its validity and reliability were more than 0.7 and 0.8, respectively. It consists of different sections that assess life, personal, health, and organizational stresses. Since, most of the study participants were housewives and we could not evaluate work-related stresses, organizational stresses were omitted from the questionnaire and the three other sections were evaluated. The first section consisted of 23 items that measured stresses related to personality and mental habits such as being unsatisfied with life, worry about the future, feelings of internal anxiety and guilt. The second section consisted of 16 items for measuring the level of stress in personal life (divorce, communicational and family conflicts, financial and occupational worries). The third section measures health-related stress using 17 items (20). With respect to scoring, a score of less than 5 for the 23-item personal stresses is normal, but a higher score indicates that the individual’s personality is the source of stress. In the 17-item health-related stress section, a score of less than 20 indicated that the person paid attention to health issues, scores of up to 60 show that health issues have prevented stress management, and scores of higher than 60 show that health issues are the source of stress. In life-related stresses, a score of less than 15 indicate normal stress, 15-40 show lack of satisfaction with life, and over 40 indicate severe stress, depression, and exhaustion.
Data analysis was done using descriptive (mean and standard deviation) and inferential statistics (correlation coefficient) for stress score distributions. Analytical tests were used for assessing mean differences based on demographic variables.
Results
In both groups, most participants were 31-40 years old and the duration of infertility was less than 5 years. Also, mixed factors (male and female) were responsible for infertility in both groups. Most participants in both groups had university degrees (table 1).
Table 1: Frequency (%) of some of the demographic variables in infertile women (Since you have the data of men in the table, you should write infertile women and men in the tile of the table.)
|
Female |
Male |
Variable |
|
| 2(1.2%)
112(65.5%) 55(32.2%) 2(1.2%) 171(100%) |
–
62 (39.5%) 87(55.4%) 8(5.1%) 178(100%) |
Lower than 20
21-30 31-40 41-50 Total |
Age
|
| 112(58.9)
55(28.9%) 18(9.5%) 5 (2.6%) 190(100%)
|
101(47.7%)
51(29.1%) 18(10.3%) 5(2.9%) 178(100%) |
Lower than 5
6-10 11-15 More than 16 total |
Duration of marriage
|
| 54(28.3%)
40(20.9%) 74 (38.7%) 23 (12%) 191(100%) |
48(287.4)
33(18.9%) 68 (38.9%) 26 (14.9%) 178(100%) |
male causes
Female causes mixed unknown total |
Cause of infertility
|
| 23(13.5%)
36(21%) 112(65.5%) 171(100%)
|
18(11%)
60(36.8%) 85(62.2%) 163(100%)
|
Primary
Diploma Higher total |
Education
level |
As shown in table 2 and figures 1-3, except for health-related stresses and positive perception of stress, other types of stress were higher in women.
Table 2 shows that apart from health stresses and positive perceptions of stress other types of stress are higher in women than men.
Table 2: Mean and standard deviations for obtained scores with respect to gender
| Variables | Sex
|
Mean | SD | CI | |
|
DASS |
Stress | Male | 6.28 | 4.10 | (5.65-6.90) |
| Female | 8.25 | 207.09 | (7.63-8.93) | ||
| Depression | Male | 4.66 | 3.41 | (3.54-4.58) | |
| Female | 6.62 | 4.85 | (5.92-7.33) | ||
| Anxiety | Male | 4.50 | 3.75 | (3.93-5.07) | |
| Female | 5.83 | 4.31 | (5.20-6.56) | ||
|
Perceived stress |
negative conception | Male | 9.78 | 5.04 | (9.78-9.02) |
| Female | 11.88 | 5.59 | (11.06-12.69) | ||
| Positive conception | Male | 14.93 | 5.03 | (14.17-15.69) | |
| Female | 13.59 | 4.84 | (12.89-14.30) | ||
|
Courdon stress test |
health stress | Male | 1.75 | 0.65 | (1.65-1.85) |
| Female | 1.66 | 0.58 | (1.58-1.75) | ||
| Personality stress | Male | 0.65 | 0.47 | (0.58-0.73) | |
| Female | 0.78 | 0.41 | (0.72-0.84) | ||
| Life stress | Male | 2.07 | 0.69 | (1.97-2.18) | |
| Female | 2.13 | 0.72 | (2.02-2.28) | ||
We found a significant relationship between the subscales of life stresses and personality stresses between the two groups (Table 3).
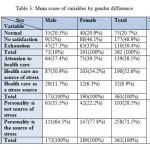 |
Table 3: Mean score of variables by gender difference |
Moreover, we found a significant relationship between the scores of all subscales of the DASS and perceived stress in both groups (table 4).
Table 4: Mean difference in DASS and perceived stress test by gender difference
|
DASS |
Variables | Sex
|
N | Mean Rank | Z | P |
| Stress | Male | 175 | 159.85 | 4.31 | 0.0001 | |
| Female | 194 | 207.09 | ||||
| Total | 369 | |||||
| Depression | Male | 175 | 155.24 | 5.10 | 0.0001 | |
| Female | 194 | 211.85 | ||||
| Anxiety | Male | 175 | 167.23 | 3.05 | 0.002 | |
| Female | 194 | 201.03 | ||||
|
Perceived stress |
negative conception | Male | 174 | 161.33 | 3.96 | 0.0001 |
| Female | 194 | 205.28 | ||||
| Positive conception | Male | 174 | 201.24 | 2.86 | 0.004 | |
| Female | 194 | 169.49 |
A significant relationship was found between sex and different variables in depression-anxiety and stress subscales and consequently positive and negative perceived stress (table 5).
Table 5: correlation between psychological distress and demographic variables
| Education | job | age | Causes of infertility | Duration of infertility | sex | variables | |
| 0.04 | 0.008 | 0.09 | 0.02 | 0.08 | 0.22* | Stress | DASS |
| 0.07 | 0.04 | 0.13# | 0.02 | 0.04 | 0.28* | Depression | |
| 0.05 | 0.02 | 0.13# | 0.01 | 0.11# | 0.17* | Anxiety | |
| 0.007 | 0.02 | 0.09 | 0.06 | 0.02 | 0.21* | Negative conception | Perceived stress |
| 0.07 | 0.02 | 0.06 | 0.06 | 0.08 | 0.12# | Positive conception | |
| 0.07 | 0.07 | 0.001 | 0.12# | 0.17* | 0.06 | Life stress |
Courdon stress test |
| 0.03 | 0.001 | 0.006 | 0.04 | 0.09 | 0.11# | Health
stress |
|
| 0.22 | 0.22 | 0.22 | 0.22 | 0.22 | 0.14* | Personality stress |
Discussion
The present study aimed to compare psychological distresses (depression, stress, anxiety, and perceived stress) and general stresses (health, personal and life stress) between infertile men and women. We found that in three subscales of the DASS (depression, stress, and anxiety) infertile women scored higher than infertile men. Moreover, when comparing general stresses, except for health related stresses, personality and life stresses were higher in women. We found a significant difference between personality stresses between the two sex groups. Other studies also showed that stress, anxiety and depression scores in the DASS were significantly higher in infertile women compared with their spouses (21, 22). Studies have indicated that women experience more psychological distresses (anxiety and depression) than men (23-27).
Other studies have also confirmed lower mental health states in infertile women and that women experience more psychological frustration with respect to infertility so that mean depression and anxiety scores are higher in women (28-31). The mental responses to infertility also differ between men and women so that women experience more mental distress (32-36).
Peterson and colleagues found that infertile women have more stress than infertile men (37). On the other hand, Andrews and co-workers found that the negative effects of infertility are considerably higher in women and women experience more mental pressure than their spouses in this regard (18). Wright also reported higher rates of psychological stress in women compared with their spouses (38).
In our study, perceived stress was assessed using the PSS-14. We found a significant difference between stress scores between men and women with respect to positive and negative perception (P<0.05). So that, a negative perception of stress was higher in infertile women and a positive perception was higher in men. These results are in line with another related study (39). Balk and colleagues also found that fertility rates increase significantly as perceived stress levels decrease (40).
Jordan and Slade also found that perceived stress which was related to infertility was significantly more in women compared with men (41, 42). Gulec also emphasizes on the different perception of women and men about infertility (43).
Other studies show no significant relationship in the type of stress based on the cause of infertility. Inconsistent with our findings, Lykeridou stated that the psychological effects of infertility could be related to the cause of infertility (44). Regardless of the fact that infertility is related to male or female factors, it has more psychological effects on women compared with men. This could be attributed to complex laboratory treatments women should undergo, even if the cause of infertility is male factors (45, 46). Ogawa found that the scores of mental disorders were lower in women who were aware of their partner’s infertility compared with those who were not (47). This is while in the present study, the cause of infertility was not related to stress.
Although, infertility affects both men and women, gender differences play a prominent role in the extent to which infertility might affect men and women (48, 49).Higher anxiety and depression rates have been observed in infertile women compared with their male counterparts (50). Other studies have also shown significant gender differences with respect to infertility related stresses (51-55).
Inconsistently, some studies did not find any gender differences with respect to depression, anxiety, and marital adaptation (56, 57). Also, when the cause of infertility is not the male factor, men’s anxiety reduces (56). Because of internal pressures (need to become a mother) and also social pressures of not having a child, mental distresses increase in infertile women. Cultural issues should also be taken into account here. For example, being a mother is an essential part of a women’s existence in many cultures (58). When men are not successful in their familial roles, they try to compensate their infertility by delving into their professional and social responsibilities. Moreover, most experiments and treatments are done on women which in turn increases their stress and decreases their self-esteem (59). Women feel more responsible with respect to infertility than men. In most societies, regardless of whether female factor is present in infertility or not, are considered responsible for infertility and feel ashamed and guilty. A women’s identity develops with the birth of a child because it is a natural and symbolic process from maturity to womanhood (60). Therefore, considering the mentioned results, the negative perceived stress in women can be explained.
One of the limitations of this study was the stress-inducing role of the unknown environment and environment related stress. Also, the number of the questionnaires and their correct completion was another shortcoming; although the participants were given enough time to complete the questionnaires. It is suggested that future research focus of family and social support on stresses experienced by infertile men and women. Also, the effect of failed treatment and couples’ stress could be studied.
Conclusion
Considering the various psychological problems in infertile couples, it is evident that infertility has a significant impact on couples over time. Mental health professionals can educate couples regarding the effectiveness of coping strategies as well as stress management techniques while experiencing the stress of infertility.
References
- Ramezanzadeh F, Noorbala A , Malak Afzali H , Shariet M , Sohrabpoor F , Bagheri M. Effective- ness of psychiatric and counseling interventions on infertility couples .Tehran University Medical Journal. 2007; 65(8): 57-63. [Persian]
- Boivin J, Bunting L, Collins J, Nygren K. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod 2007 march; 22(6): 1506-1512
- Covington SN, Hammer Burns L. Infertility counseling.2nd ed. New York: Cambridge University Press; 2007 . p.1- 17, 175-180, 493-506
- دکتر کمالی محمد و همکاران، بررسی اپیدمیولوژیک علل ناباروری در بیماران مراجعه کننده به پژوهشکده رویان، مجله پزشکی دانشگاه علوم پزشکی تبریز، دوره 8 شماره 1 بهار 1385 صفحات 103-105
- Shapiro CH. Therapy with infertile Heterosexual couples: It’s not about gender-or is it?. Clin Soc Work J 2009;37:140-9.
- Vahidi S, Ardalan A, Mohammad K. The epidemiology of primary infertility in the Islamic Republic of Iran in 2004-5. Reprod Infertil J 2007;7(3):243-51.
- Smeenk JM., Verhaak CM, Vingerhoets AJ, Sweep CG, Merkus JM, Willemsen SJ, et al. Stress and outcome success in IVF: the role of self-reports and endocrine variables. Hum Reprod 2005 Apr;20(4):991-6.
- Monga M, Alexandrescu B, Katz SE, Stein M. Impact of infertility on quality of life, marital adjustment and sexual function. Urology 2004;63126-30.
- Johnston WI, Oke K, Speirs A, et al. Patients selection for invitro fertilization: physical and psychological aspects. Annual of NewYork Academic Science 1985; 442: 490-503
- Nelson, C. J., Shindel A. W., Naughton, C. K., Ohebshalom, M., & Mulhall, J.P. (2008). Prevalence and predictors of sexual problems, relationship stress, and depression in female partners of infertile couples. Journal of Sexual Medicine.5(8):1907-14
- Zhao, L. M., Jiang, H., Sui, Y. J., Tang, W. H., Yuan, R. P., & Ma, L. L. (2007). An approach to male infertility from economic sociology. Zhonghua Nan Ke Xue. 13(9):795-7. [Article in China].
- Keyes, Corey L. M. & Goodman, Sherryl H. (2006). Women and Depression: A handbook for the social, behavioral and biomedical sciences. New
- Wischmann T. Psychological factors in infertile women. J Urologe A. 2005 Feb; 44(2): 185-94.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther.1995 ;33:335–343.
- Lovibond SH, Lovibond PF. Manual for the Depression-Anxiety-Stress Scales . Sydney, New South Wales, Australia: The Psychology Foundation of New South Wales Inc, University of New South Wales;1995 .
- Clara I, Cox B, Enns M. Confirmatory factor analysis of the Depression-Anxiety-Stress Scales in depressed and anxious patients. J Psychopathology & Behav Assess.2001 ;23:61–67
- Brown TA, Chorpita BF, Korotitsch W, Barlow DH. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav Res Ther.1997 ;35:79–89.
- Antony M, Bieling P, Cox B, et al. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales (DASS) in clinical groups and a community sample. Psychol Assess.1998 ;10:176–181.
- Cohen S. Contrasting the hassle scale and the perceived stress scale. American Psychologist 2003, 41, 716-719.
- Ganji H. Textbook of character evaluation. 3rd ed. Savalan Publisher; 2005. pp. 217–25.
- Ramli M et al. A preliminary study of the psychological differences in infertile couples and their relation to the coping styles.comprehensive psychiatry 55(2014)565-569.
- Drosdzol A, Skrzypulec V. Depression and anxiety among Polish infertile couples; an evaluative prevalence study. J Psychosom Obstet Gynaecol 2009;30(1):11-20.
- El Kissi Y,Ben Romdhane A, Hidar S, Bannour S, Ayoubi Idrissi KH, Khair H, Ben Hadj Ali B. General psychopathology, anxiety, depression and self-esteem in couples undergoing infertility treatment: a comparative study between men and women. European Journal of Obstetrics & Gynecology and Reproductive Biology 167 (2013) 185–189.
- Wichman C, Ehlers S, Wichman S, Weaver A, Coddington C. Comparison of multiple psychological distress measures between men and women preparing for in vitro fertilization. Fertility and Sterility 2011;65:717–21.
- Chiaffarino F, Baldini M, Scarduelli C, et al. Prevalence and incidence of depressive and anxious symptoms in couples undergoing assisted reproductive treatment in an Italian infertility department. European Journal of Obstetrics Gynecology and Reproductive Biology 2011;158:235–41.
- Lechner L, Bolman C, van Dalen A. Definite involuntary childlessness: associations between coping, social support and psychological distress.Hum Reprod 2007;22:288–294.
- Lund R, Sejbaek CS, Christensen U, Schmidt L. The impact of social relations on the incidence of severe depressive symptoms among infertile women and men. Hum Reprod 2009;24:2810–2820.
- Burns, L. H., & Covington, S. N. (2000). Inefrtility counseling: A Comprehensive Handbook for Clinicians. New York: Purthenon.
- Matsubayashi, H., Hosaka, T., Izumi, S., Suzuki, T., Kondo, A. & Makino, T. (2004). Increased depression and anxiety in infertile Japanese women resulting from lack of husband’s support and feelings of stress. General Hospital Psychiatry. 26 (5). 398-404.
- Wischmann, T., Scherg, H., Strowitzki, T., & Verres, R. (2009). Psychosocial characteristics of women and men attending infertility counselling. Human Reproduction. 24(2):378-85.-
- Weiss, P., Mateju, L., & Urbanek, V. (2004). Personality and characteristics of couples in infertile marriage. Ceska Gynekologie. 69 (1). 42-47.
- Chachamovich J, Chachamovich E, Ezer H, Fleck M, Knauth D, Passos E. Investigating quality of life and health-related quality of life in infertility: a systematic review. J Psychosom Obstet Gynaecol 2010;31:101–110.
- Lund R, Sejbaek CS, Christensen U, Schmidt L. The impact of social relations on the incidence of severe depressive symptoms among infertile women and men. Hum Reprod 2009;24:2810–2820
- Ragni G, Mosconi P, Baldini MP, Somigliana E, Vegetti W, Caliari I, Nicolosi AE. Health-related quality of life and need for IVF in 1000 Italian infertile couples. Hum Reprod 2005;20:1286–1291.
- Rashidi B, Montazeri A, Ramezanzadeh F, Shariat M, Abedinia N, Ashrafi M. Health-related quality of life in infertile couples receiving IVF or ICSI treatment. BMC Health Serv Res 2008;8:186.
- Verhaak CM, Lintsen AME, Evers AWM, Braat DD. Who is at risk of emotional problems and how do you know? Screening of women going for IVF treatment. Hum Reprod 2010;25:1234–1240.
- Peterson B.D, Pirritano M, Christensen U, Boivin J, Block J , Schmidt L. The longitudinal impact of partner coping in couples following 5 years of unsuccessful fertility treatments. Human Reproduction 2009;Vol.24, No.7 pp. 1656–1664.
- Andrews, F. M., Abbey, A., & Halman, L. J. (1992). Is fertility problem stress different? Fertility and Sterility, 57, 1247-1253.
- Wright, J. D. (1991). Psychological distress and infertility men and women respond diffrently. Fertility and Sterility, 55, 100-108.
- Christopher R. Newton, Wendy Sherrard, Irene Glavac. The Fertility Problem Inventory: measuring perceived infertility-related stress. FERTILITY AND STERILITY (JULY 1999);VOL. 72, NO. 1.
- Balk J, Catov J, Horn B, Gecsi K, Wakim A. The relationship between perceived stress, acupuncture, and pregnancy rates among IVF patients: A pilot study.Complementary Therapies in Clinical Practice 16 (2010);154–157.
- Jordan C, Revenson TA. Gender differences in coping with infertility: a meta-analysis. J Behav Med 1999;22(4):341-58.
- Slade P, O’Neill C, Simpson AJ, Lashen H. The relationship between perceived stigma, disclosure patterns, support and distress in new attendees at an infertility clinic. Hum Reprod 2007;22(8):2309-17.
- GULEC G, HASSA H, GUNEŞ E, YENİLMEZ C. Th e Eff ects of Infertility on Sexual Functions and Dyadic Adjustment in Couples that Present for Infertility Treatment. Turkish Journal of Psychiatry 2011; 22( ).
- Lykeridou K, Gourounti K, Deltsidou A, Loutradis D, Vaslamatzis G. Theimpact of infertility diagnosis on psychological status of women undergoing fertility treatment. J Reprod Infant Psychol 2009;27:223–237.
- Ozcelik B, Karamustafalıoğlu O, Ozcelik A (2007) İnfertilitenin psikolojik ve psikiyatrik yonu. Anadolu Psikiyatri Dergisi, 8: 140- 148.
- Repokari L, Punamaki RL, Unkilo-Kallio L et al. (2007) İnfertility treatment and marital ralationships: A 1 year prospective study among successfully treated ART couples and their controls. Hum reprod, 22: 1481- 1491.
- Ogawa M, Takamatsu K, Horiguchi F.Evaluation of factors associated with the anxiety and depression of female infertility patients.Biopsychosocial medicine 2011, 5:15.
- Monga M, Bogdan A, Katz SE, Stein M, Ganiats T. Impact of infertility on quality of life, marital adjustment and sexual function. Urology 2004;63:126–30.
- Guliz O , Nezihe Kizilkaya B. Effects of infertility on gender differences in marital relationship and quality of life: a case-control study of Turkish couples, European journal of obstetrics & gynecology and reproductive biology 165(2012)243-248.
- McQuillan J, Rosalie A, Stone T, et al. Infertility and life satisfaction among women. J Fam Issues 2007;28(7):955-81.
- Abedinia, N., Ramazanzadeh, F., & Aghssa, M. M. (2003). Relationship between anxiety and depression with duration of pregnancy. Quartenaryy Journal Payesh, 4, 153–158.
- Lee, T. Y., Sun, G. H., & Chao, S. C. (2001). The effect of an infertility diagnosis on the distress, marital and sexual satisfaction between husbands and wives in Taiwan. Human Reproduction, 16, 1762–1767.
- Schmidt L, Holstein B, Christensen U, Boivin J. Does infertility cause marital benefit? An epidemiological study of 2250 women and men in fertility treatment. Patient Educ and Couns 2005;59:244–251.
- Galhardo A, J. Pinto-Gouveia, M. Cunha & Matos. “The impact of shame and self-judgment on psychopathology in infertile patients”, Human Reproduction, Vol 26 (9), (2010).
- TUZER V et al. Marital adjustment and emotional symptoms in infertile couples: gender differences Turk J Med Sci 2010; 40 (2): 229-237.
- Karlidere T, Bozkurt A, Yetkin S, Doruk A, Sutcigil L, Ozmenler KN et al. Is there gender difference in infertile couples with no axis one psychiatric disorder in context of emotional symptoms, social support and sexual function? Turk Psikiyatri Dergisi 2007; 18: 311-322.
- Alizadeh T, Farahani MT, Shahr Aray M, Alizadegan S. The relationship between self esteem and locus of control with stress in infertile women and men. J Reprod Fertil. 2005; 5(19) 194-204.
- Zorn B, Auger J, Velikonja V, Kolbezen M, Meden-Vrtovec H. Psychological factors in male partners of infertile couples: relationship with semen quality and early miscarriage. Int J Androl. 2008; 31(6): 557-564.
- Abbey F, Andrews M, Hallmant L. Infertility and subjective well being: The mediating roles of self esteem, internal control and interpersonal conflict. J Marriage Fam.1992; 54(2): 408- 417.

This work is licensed under a Creative Commons Attribution 4.0 International License.



