

How to Cite | Publication History | PlumX Article Matrix
Ambulance Technical Actions’ Skills of Iranian Freshman Emergency Medical Students in 2014
Rohollah Mohammadi1, Marzieh Seidabadi2*, Shokrollah Abumaash Zadeh3, Rohangiz Norouzinia4, Yaser Mohammadi5, Ali Mohammadi6
1MSc. Emergency Medical Department, Kermanshah University of Medical Sciences, Kermanshah, Iran 2MSc. Emergency Medical Department, tutor of Paramedics, Alborz University of medical science, Karaj, Iran 3BSc. Emergency Medical Department, Tutor of Paramedics, Alborz University of medical science, Karj, Iran. 4MSc. Research and Development of medical science Education Center, Alborz University of medical science, Karaj, Iran 5Young Researchers Club, Islamic Azad University, Karaj Branch, Karaj, Iran 6Health Information Technology Department, faculty of Paramedicine, Kermanshah University of Medical Sciences, Kermanshah, Iran
DOI : http://dx.doi.org/10.13005/bbra/1941

ABSTRACT: Working in emergency fields potentially needs high theoretical and practical abilities; because making creative decision and implementing therapeutic intervention have to do as soon as possible, so that patience life won’t in threat. Thus, this study aimed to evaluate the level of Skills and knowledge of bachelor freshman Emergency Medical Students about ambulance technical actions in 2014. A descriptive- analytical study was conducted on 146 Iranian freshman students who newly admitted for emergency medical Bachelor’s degree in Alborz medical science university in 2014. Students' knowledge and skill of ambulance technical actions were measured through a visual checklist including 4 main actions that totally encompassed 13 technical actions and each action had a maximum score to gain. Data was analyzed by the SPSS software through one-sample t- test statistical test. The results revealed that students’ skill and knowledge about ambulance technical actions was in moderate level. Also, there was a significant difference between their received score and maximum score of knowledge. As a result, an expected and comprehensive knowledge about ambulance technical actions and the order of actions was not observed, as the current situation of students’ knowledge and skills was lower than optimal knowledge up to 10.404 scores. Considering the lack of expected knowledge and skills of students about ambulance technical actions which observed in this study, it is concluded that their information has forgotten over time and therefore, recommended to retrain students and increase practical courses on ambulance technical actions in universities.
KEYWORDS: Ambulance Technical Actions; Students’ skill and knowledge; Emergency medical services; Iran
Download this article as:| Copy the following to cite this article: Mohammadi R, Seidabadi M, Zadeh S. A, Norouzinia R, Yaser Mohammadi Y, Mohammadi A. Ambulance Technical Actions’ Skills of Iranian Freshman Emergency Medical Students in 2014. Biosci Biotechnol Res Asia 2015;12(3) |
| Copy the following to cite this URL: Mohammadi R, Seidabadi M, Zadeh S. A, Norouzinia R, Yaser Mohammadi Y, Mohammadi A. Ambulance Technical Actions’ Skills of Iranian Freshman Emergency Medical Students in 2014. Biosci Biotechnol Res Asia 2015;12(3). Available from: https://www.biotech-asia.org/?p=2402 |
Introduction
Primary prevention continues to be one of the most important ways to reduce the burden of injuries and damages while evidence showed that many of the deaths and long-term disabilities are preventable by strengthening trauma and emergency care [1,2]. The history of modern out-of-hospital emergency medical services (EMS) go back to the 1960s and 1970s when some brave medical personnel go out of hospitals and later published their successful experiences with lifesaving services about treating acute coronary syndromes, trauma care, and cardiopulmonary arrest on-scene [3-5]. Todays, Prehospital medical cares (115 emergency medical) are the critical part of health services provision system which should be simple, continuous and efficient [6]. They play an important role in treatment-health network and have vital contribution to provide prehospital services and patients’ movement into medical treatment centers [7].
The quality of prehospital EMS is directly related to survival rate, as whatever the quality increase, the rate of survivable is improved [8-12]. This means that, working in emergency fields potentially needs high theoretical and empirical abilities; because making creative decision and implementing therapeutic intervention have to do as soon as possible, so that patience life won’t in threat [13-14]. For a reason that it may be a lot of people who needs Cardiopulmonary Cerebral resuscitation (CPCR), knowledge and skill about that is necessary even for common people [15]. Hunskaar and Seim recommended that all medical school graduates acquire skills in emergency life-saving procedures [16-17].
Paramedic skill portfolios ranged from basic skills of working with ambulance to the more advanced skills of electrocardiographic (EKG) interpretation, defibrillation attempts etc[5,18]. Ambulance services is provided worldwide for more than a century [19] and helped human to transfer patients to medical care centers rapidly.
It may not be clear what kind of skills are needed for the next emergency patient but what is really indispensable in all emergency cases is having skill to work with ambulance and use their service because the ambulance would need to experience nearly 10,000 EMS incidents a year overall [5]. On the other hand, for emergency and accident units, the possible shortest time to provide basic life supports are noteworthy and advanced ambulance service is considered to be an integral part of emergency medical care as the first assets responding to emergencies and disasters in the prehospital setting in most developed countries [20-21]. It is well known that survival for patients with out-of-hospital cardiac arrest is dependent on their receiving treatment within a very short time frame [22-25].O’Keeffe et al. (2010), estimated that a 1 min reduction in ambulance response times would save approximately 149 lives per year and that each survivor would achieve 3.72 quality-adjusted life years [23]. But it should be mentioned, besides, shortest response time by ambulance, other factors like rapid EMS response, well-trained personnel and case attributes are important as well [26-28]. Certainly, ambulance per se is not panacea and this is personnel’ skill and knowledge to know about technical actions and treat patients on the ambulance which are mainly expeditious.
Therefore, considering importance of emergency medical services (EMS) personnel skills toward ambulance technical actions, an attempt was therefore made to test the theoretical and practical ability of Iranian freshman emergency medical students based on the standard guidelines of ambulance technical actions (ATA) to figure out how big the gap between their current and optimal skills is.
Methods
Research method and samples
A descriptive- analytical study was conducted. The subjects included 146 Iranian freshman students who newly admitted for emergency medical Bachelor’s degree in Alborz medical science university in 2014. The number of 146 students were calculated using Cochran’s formula and selected randomly.
The inclusion and exclusion criteria were as follow
Inclusion criteria included all students who had passed the course of ambulance technical actions in the previous educational section and were voluntarily satisfied to participate in this study. Exclusion criteria also was the lack of willing to participate and continue in this study. All study procedures were explained to the students, and they were participated after obtaining their informed consent.
Materials and study process
Data were collected through a questionnaire of demographic information (age, marital status, being employment, work experience, work setting, the previous university, the average score, the status of interest, knowledge and attitudes toward their field of study) and a standard checklist including a set of guidelines for the performance of ambulance technical actions has been formulated by American Heart Association (AHA) [28].
While students had attended Alborz medical university to register in new curriculum, the questionnaires were distributed randomly among them after describing study procedures and how they have to ask question. The response rate of questionnaires was 100%.
Students’ attitudes towards their field of study also were measured by a scale of 13 items covering Strengths and weaknesses of emergency medical curriculum and asked them to answer based on Likert scale ranged from 1 = strongly disagree to 5 = strongly agree.
To measure students’ knowledge and skill about ambulance technical actions stages, a standard checklist containing 4 main actions that totally encompassed 13 technical actions were used in which each action had a maximum score if correctly and rapidly be answered.
The content validity of questionnaires were confirmed by opinions of 10 experts who were known in this field of study. The reliability of them also were confirmed through estimation Cronbach alpha coefficient (ά =0.91) for 30 students were participated in a pretest. This students were apart of sample students but theirs status were the same of sample group.
Students’ knowledge and skill about ambulance technical actions was measured theoretically and practically as fallow: at the first, they were asked to answer the questions of checklist about technical actions correctly and then in practical phase, they were requested to show the location and signs of each action on the ambulance and to perform some actions practically. Each action had a maximum score while be done correctly and the total optimal score for all actions was 26. In the next stage, the actual score of students for each action and total score for all actions were calculated and compared to optimal (maximum) score. As a result, students with skill score under 15 were categorized as low skillful, between 15.1 to 20 and over 20.1 as moderately and highly skillful respectively. Finally the total gained score of students’ skill were compared to the optimal score of checklist using one sample t test trough SPSS software.
Results
The majority of participants aged 30 to 35 years and were married. About 97 percent of them were employment and only 3 percent were unemployment. Most of them (62.3%) had more than 5 years’ work experiences and worked (93%) in 115 emergency bases and the rest worked in hospitals (5.5%) and private emergencies (1.5%). Average score of them ranged 15 to 17 mostly (table 1).
Table 1: Frequency distribution of the majority classes of studied variables
| variables | The majority class | frequency | percent |
| Age range | 30-35 | 73 | 50 |
| Marital status | Married | 106 | 72.6 |
| Employment status | Employment | 142 | 97.3 |
| Work experience | > 5 years | 91 | 62.3 |
| Work setting | 115 emergency base | 136 | 93.2 |
| The average score | 15-17 | 95 | 65.1 |
Also, the results showed that the majority of students (92.5%) had high and very high familiarity with their field of study and the rest had moderate (6.2%), low (0.7%) and without (0.7%) familiarity. Moreover, according to students’ interest about their field of study results, the majority (94.5%) had high and very high interest about their field of study and only 0.7 percent of them had no interest about their field of study (Table 2).
Table 2: Frequency distribution of studied students based on familiarity and interest about their field of study
| variables | None | Low | moderate | high | Very high | |||||
| Frq. | Pct. | Frq. | Pct. | Frq. | Pct. | Frq. | Pct. | Frq. | Pct. | |
| Familiarity with their field of study | 1 | 0.7 | 1 | 0.7 | 9 | 6.2 | 63 | 43.2 | 72 | 49.3 |
| Interest about their field of study | 1 | 0.7 | 0 | 0.0 | 7 | 4.8 | 41 | 28.1 | 97 | 66.4 |
Frq. = frequency Pct. = Percent
Students’ Attitude toward their emergency medical curriculum
According to research findings, the majority of students (95.8%) were agree and strongly agree toward their emergency medical curriculum. In other word, most of them had positive attitudes toward their field of study and no one had negative attitude. The mean and standard deviation of attitude value was 4.12 ± 0.406 which showed that participants’ attitudes were into positive range (Table 3).
Table 3: Frequency distribution of Participants’ attitude towards their emergency medical curriculum
| Attitude toward emergency medical curriculum | frequency | percent | Mean ± SD | Min. | Max. |
| Strongly disagree | 0 | 0.0 | 4.12 ± 0.406 | 2.92 | 4.85 |
| Disagree | 0 | 0.0 | |||
| No opinion | 6 | 4.1 | |||
| Agree | 103 | 70.5 | |||
| Strongly Agree | 37 | 25.3 | |||
| Total | 146 | 100.0 |
Scale range: Strongly disagree = 1, Disagree =2, No opinion = 3, Agree = 4, Strongly Agree = 5
Ambulance technical actions’ skills of emergency medical students
Evaluating theoretical and practical skills of students about ambulance technical actions procedure showed that their mean score of total skills was about 21 which was significantly lower than optimal score of 26 and a gap of 5 score were seen. However, they were totally situated in moderate-high skill category according to this score. Moreover, as mentioned above, emergency medical students were categorized into three groups based on their skill level as fallow: the low skill group whose score was under 15 and contained about 13 percent of students; The moderate skill group whose score ranged from 15.1 to 20 which were about 25 percent and the high skill group whose gained score was more than 20.1 and contained about 62 percent of students (table 4).
Table 4: Frequency distribution of students based on their ambulance technical actions’ skills
| skills level and score | Frq. | Pct. | Cum. Frq. | Mean ± SD | Min. | Max. |
| *X ≤ 15 (low skill level) | 19 | 13.0 | 13.0 | 20.9 ± 4.24 | 8 | 26 |
| 15.1 ≤ X ≤ 20 (moderate skill level) | 37 | 25.4 | 38.4 | |||
| X ≥ 20.1 (high skill level) | 90 | 61.6 | 100.0 | |||
| Total | 146 | 100.0 |
*X= Skill score gained by students; Frq. = frequency; Pct. = Percent
However, the majority of students had acceptable skill but according to comparing mean score of total studied population’ skill with maximum (optimal), students’ skill were significantly far from optimal and there was not proficiency with ambulance technical actions. In addition, based on “t value” and its minus sign, confidently can be said that there is a significant gap of 5.10 between actual gained skill and optimal skill (Table 5).
Table 5: Compare mean of students’ ambulance technical actions’ skill with optimal score
| actual ambulance technical actions’ skill | Mean score gained | Optimal score | t value | Sig. | Mean Difference | 95% Confidence Interval of the Difference | |
| Lower | Upper | ||||||
| 20.93 | 26 | -14.46** | 0.000 | -5.07 | -5.76 | -4.38 | |
** Significant at 99% level
The results of evaluating students’ knowledge and skills about all actions one by one also showed that there was significant gap between actual skill score of all actions with their optimal score. This means that there was no action which could be done properly by all students. However, some actions had more gaps and some had less which realized that the level of students’ skills differ from one action to another. Indeed, the more actions were close to the optimal level, the more students were update and proficiency.
Knowing which main actions and sub-actions were theoretically and practically performed properly, a gap analysis was done and all actions were ranked through mean differences factor.
The results of the ranking showed that, among four main actions, the “color signs on the kilometer unit” main action was ranked first (A rank) which means that this main action had the lowest gap between actual skill and optimal skill of students. In other word, students had the highest familiarity with this item, knowing these color signs and how they work. The second rank (B rank) was belong to “changing stretcher position properly” main action which revealed that students’ skill about that was lower than color signs on the kilometer unit but better than other two main actions of “Acceleration Skid Regulation (ASR)” and “ambulance morning checking “ which ranked third (C rank) and fourth (D rank) respectively. Considering the ranking, checking the ambulance in the morning and before using was the worst action among four main action based on student’s skill. It may be attributed to this fact that the action is more technical than other main actions and maybe they supposed that this checking is only ambulance driver duty (Table 6).
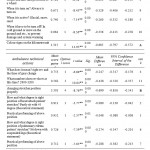 |
Table 6: Compare mean of students’ actual ambulance sub-technical actions’ skill with optimal score |
The ranking of sub-technical actions based on their mean differences (skill gap), also showed that, “practically put heart attack patient in the right position on the stretcher” and “theoretically being aware of what position is proper for heart attack patient on the stretcher” with mean differences of -0.048, and -0.089 were ranked first and second respectively. In other word, against other sub-technical actions, these two were done more correctly by students and a little distance was seen between actual gained skill and optimal needed skill. Reversely, sub-actions of checking “ambulance body, radiator water, engine oil, brake oil, hydraulic oil of drive, battery and engine” and “windshield washing water, windshield wiper blades, belts, trailer, engine test, gearbox test, moving ambulance a bit forward and backward, air filter, glasses and mirrors” with mean differences of -1.082 and -2.205 were ranked at the lowest level respectively which means that students had least knowledge and skill about these actions and couldn’t perform them correctly. The other ranking results are observable in table 6.
Discussion
Resuscitation of victims can be improved with early access, early cardiopulmonary resuscitation (CPR), early defibrillation, early advanced care and post-resuscitation care [30-31]. Immediate treatment implies a survival chance of approximately 67 percent, while the decline in survival rate without treatment is 5.5 percent per minute and after 12 minutes a patient does not survive [32]. Thus, survival is extremely time-sensitive, so, organization of the emergency medical services (EMS) and other resources involved in the process like ambulance and properly trained personnel with high skill level to work with ambulance is critical [33]. The lack of awareness about operations on the ambulance and its technical actions lead to delay in call response and insufficient treatments.
With this in mind, this study was aimed to answer two main questions: how update the knowledge and skills of emergency medical students -who newly admitted to Alborz medical university of Iran and passed the ambulance technical actions courses before- is? Is hiatus after passing ambulance technical actions courses in classroom affect negatively on the students’ knowledge and skill? Therefore, theoretical knowledge and practical skill of students was evaluated using ambulance technical actions checklist on two ambulances.
The results of demographic characteristics of students showed that all students except three percent of them were working particularly in 115 emergency bases for more than 5 years. However some of them were working in hospitals and private emergencies. These means that they were involving in emergency care services and weren’t much far from life-saving activities. Also, they were really interested in your field of study and had positive attitudes towards emergency medical services and curriculum. Therefore, it was assumed that students’ knowledge and skills of ambulance technical actions is updated without significant distance to optimal one.
According to results of students’ knowledge and skill about ambulance technical actions, however, they averagely gained 21 out of 26 (optimal score) and were categorized as students with moderate-high skill, but this gap between actual gained skill and optimal skill was statistically significant. In other word, can be said that there were fluctuations among students in case of their knowledge and skill about ambulance actions as some of them were highly skillful and the others were semi skillful or skilless. Therefore, according to results, hiatus after passing courses in classroom affected negatively on the students’ knowledge and skill. Pepe (2015) also stated that skills may deteriorate a little with a hiatus from practice. Moreover, Even if initial training techniques are expert and well-taught, both in the classroom and on-scene, frequency of performance is a critical factor [5]
The next important result deducted from gap analysis and ranking procedure was that, with moving to more technical actions, the students’ skill go down and reversely. In other word, they had forgotten the actions were related to machine technical actions more than those of patient-related. For example, the least gap between actual skill and optimal level was observed for two actions related to properly changing the heart attack patient’ position on the stretcher in both theoretical and practical dimensions which means that their knowledge about how they treat with injured patient was acceptable. But, on the other hand, the most gap was belong to main action of checking ambulance in the morning which contains checking either ambulance body, radiator water, engine oil or windshield wiper blades, belts, trailer and engine test. Also, they had a volatile memory in case of ambulance ASR which was related to anti-skid system definition and how it works. Therefore, they were aware of actions attributed to patient treatment because these actions experienced frequently for them but they seldom check the ambulance technical specifications like engine oil or radiator water. In other word, students’ technical know how about ambulance was not as high as it have to be. Another reason can be arise from this thought that, ambulance technical standards and services is not emergency medical personnel’ duty or maybe are not as important as patient-related services are.
In total, what is really important is that low skills of emergency medical student led to low quality of life support procedures and when the quality of emergency medical cares is poor, survival rates are decreased.[34] Therefore, attention to training programs and methods both theoretically and practically by experts are really essential because the efficacy of resuscitation can be maximized when EMS practitioners develop and maintain competency in the skills and knowledge of resuscitation by more training [35]. In addition, resuscitation skills usually deteriorate rapidly after training [12-36]. Thus, the training of EMS personnel in the skill of ambulance technical actions should be given high priority.
The effective training programs in order to improve students’ knowledge and skill and maintain update must fallow some points such as: first, Training and experience are more important than the type of practitioner for success.[37] Moreover, learning activities pursued by the student must correct weaknesses and improve performance, and must be coupled with immediate feedback, correction, remediation and repetition.[17] Second, the methods used to train paramedics in ambulance services should re-examine.[38] Third, the training programs must repeat frequently with update information. With increasing quality of training programs, the emergency medical personnel’ skill improve and subsequently the rate of survival increase [39].
Acknowledgements
The authors thank the participants for taking part in this study in particular the assistance of emergency medical department of Alborz medical science university.
References
- Haghani F, Sadeghi N. Training in Pre-hospital Emergency: Needs and Truths. Iran J. Med. Educ. 2010; 10: 1273-1280.
- Mock C, Abantanga F, Goosen J, Joshipura M, Juillard C: Strengthening care of injured children globally. Bull World Health Organ. 2009; 87: 382-389.
- Cobb LA, Alvarez H, Copass MK: A rapid response system for out-of-hospital cardiac emergencies. Clin. North. Am. 1976; 60: 283–93.
- Pantridge JF, Geddes JS. A mobile intensive care unit in the management of myocardial infarction. Lancet. 1967; 290: 271–3.
- Pepe PE, Roppolo LP, Fowler RL. Prehospital endotracheal intubation: elemental or detrimental? Critical Care. 2015; 19: 121- 8.
- Eskrootchi R, Ebadi Fard A, Abolhassani H, Kahouei M. A survey on medical students needs in Iran University of medical sciences emergency clinical education. J Health Admin. 2008; 11(33): 69-76.
- Luiz T. Emergency medicine tomorrow. Anesthesiology, Intensive medicine, Not fall medicine, Schemers therapy: AINS. 2003; 38(4): 296-302.
- Christenson J, Andrusiek D, Everson-Stewart S, Kudenchuk P, Hostler D, Powell J, et al. Chest compression fraction determines survival in patients with out-of-hospital ventricular fibrillation. Circulation. 2009; 120: 1241–7.
- Steen PA, Kramer-Johansen J. Improving cardiopulmonary resuscitation quality to ensure survival. Opin. Crit. Care. 2008; 14: 299–304.
- Idris AH, Guffey D, Aufderheide TP, et al. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation. 2012; 125: 3004–12.
- Kramer-Johansen J, Myklebust H, Wik L, et al. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback: a prospective interventional study. Resuscitation 2006; 71: 283–92.
- Dysona K, Braya J, Smitha K, Bernarda S, Finn J. A systematic review of the effect of emergency medical service practitioners’ experience and exposure to out-of-hospital cardiac arrest on patient survival and procedural performance. Resuscitation. 2014; 85: 1134–1141.
- Franklin A, Liu Y, Li z, Nguyen V, Johnson T, Robinson D, et al. Opportunistic decision making and complexity in emergency care. Biomed. Inform. 2011; (44): 469-476.
- Dy S, Purnell T. Key concepts relevant to quality of complex and shared decision making in health care: Literature review. Sci. & Med. 2012; (74): 582-587.
- Kayama M, Akiyama T, Ohashi A, Horikoshi N, Kido Y, Murakata T, Kawakami N. Experiences of Municipal Public Health Nurses Following Japan’s Earthquake, Tsunami, and Nuclear Disaster. Public Health Nurs. 2014; 31: 517-25.
- Hunskaar S, Seim SH. Medical students’ experiences in medical emergency procedures upon qualification. Educ. 1985; 19(4): 294-8.
- Tarasi PG, Mangione MP, Singhal SS, Wang HE: Endotracheal intubation skill acquisition by medical students. Educ. Online. 2011; 16: 7309 – DOI: 10.3402/meo.v16i0.7309
- Page JO. The paramedics: an illustrated history of paramedics in their first decade in the U.S.A. Morristown, New Jersey, USA: Backdraft Publications; 1979.
- McManus WF, Tresch DD, Darin JC. An effective prehospital emergency system. J Trauma. 1977; 17: 304–10.
- Farshi M, Babatabar Darzi H, Mahmoudi H, Mokhtari Nouri J. Comparison of nursing care learning in airevacuation and transport by lecture and e-learning methods. J. Mil. Med. 2012; 4(1): 27-31.
- Peyravi M, Örtenwal P, Djalali A, Khorram-Manesh A. An Overview of Shiraz Emergency Medical Services, Dispatch to Treatment. Red Cres. Med. J. 2013; 15(9): 823-8. DOI: 10.5812/ircmj.10982.
- De Maio V, Stiell I, Wells G, et al. Optimal defibrillation response intervals for maximum out of hospital cardiac arrest survival rates. Ann Emerg Med. 2003; 42: 242-50.
- O’Keeffe C, Nicholl J, Turner J, Goodacre S. Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emerg Med J. 2010; 1-4.
- Blackwell TH, Kaufman JS. Response time effectiveness: comparison of response time and survival in an urban emergency medical services system. Emerg. Med. 2002; 9: 288.
- Pell JP, Sirel JM, Marsden AK, Ford I, Cobbe SM. Effect of reducing ambulance response times on deaths from out of hospital cardiac arrest: cohort study. BMJ. 2001; 322: 1385-8.
- Herlitz J, Engdahl J, Svensson L, et al. Factors associated with an increased chance of survival among patients suffering out of hospital cardiac arrest in a national perspective in Sweden. Am Heart J. 2005; 149: 61-6.
- Kette F, Sbrojavacca R, Rellini G, et al. Epidemiology and survival rate of out of hospital cardiac arrest in North East Italy: the F.A.C.S. study. Fruili Venezia Guilia Cardiac Arrest Co-operative Study. Resuscitation. 1998; 36: 153-9.
- Klepeis P. The availability of ambulance services in Madison County, NY. Middle States Geographer. 1993; 26: 58-66.
- Irwin RS, Rippe JM, Lisbon A: Intensive Care Medicine. 5th ed. St Louis: Lippincott and Wilkins; 2008.
- Cummins RO, Ornato JP, Thies WH. & Pepe PE. Improving survival from sudden cardiac arrest: the ‘chain-of-survival’ concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation. 1991; 83: 1832-1847.
- Hollenberg J, Lindqvist J, Ringh M, Engdahl J, Bohm K, Rosenqvist M. & Svensson L. An evaluation of post-resuscitation care as a possible explanation of a difference in survival after out-of-hospital cardiac arrest. 2007; 74: 242-252.
- Larsen MP, Eisenberg MS, Cummins RO, Hallstrom AP. Predicting survival from out-of-hospital cardiac arrest: a graphic model. Emerg. Med. 1993; 22: 1652–1658.
- Sund B. The value of a statistical life for out-of-hospital cardiac arrest victims. Örebro University Swedish Business School, Working Paper Series, 2010:4.
- Sasson C, Mary AM, Rogers MAM, Dahl J, Kellermann AL. Predictors of Survival from Out-of-Hospital Cardiac Arrest A Systematic Review and Meta-Analysis. Circ Cardiovasc Qual Outcomes. 2010; 3: 63-81.
- Soar J, Mancini ME, Bhanji F, Billi JE, Dennett J, Finn J, et al. Part 12: Education, implementation, and teams: 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2010; 81: e288–332.
- Yang CW, Yen ZS, McGowan JE, Chen HC, Chiang WC, Mancini ME, et al: A systematic review of retention of adult advanced life support knowledge and skills in healthcare providers. Resuscitation. 2012; 83: 1055–60.
- Fouche PF, Middleton PM, Zverinova KM: Training and experience are more important than the type of practitioner for intubation success. Critical Care. 2013; 17: 412.
- Johnston BD, Seitz SR, Wang HE: Limited Opportunities for Paramedic Student Endotracheal Intubation Training in the Operating Room. Emerg. Med. 2006; 13(10): 1051-1055.
- O’Flaherty D, Adams AP: Endotracheal intubation skills of medical students. R. Soc. Med. 1992; 85: 603- 4.

This work is licensed under a Creative Commons Attribution 4.0 International License.



