

How to Cite | Publication History | PlumX Article Matrix
Maryam Maktabi1, Afsaneh Nouruzi2, Zahra Farzinnia1 and Alireza Kamali2*
1Department of Gynecology, Arak University of Medical Sciences, Arak, Iran.
2Department of Anesthesiology, Arak University of Medical Sciences, Arak Iran.
Corresponding Author E-mail: alikamaliir@yahoo.com
DOI : http://dx.doi.org/10.13005/bbra/2401

ABSTRACT: The uterine contractions remain constant a few hours after delivery. Various studies have pointed to the fact that uterine contractions are quite similar to those contractions that result in child delivery. Various medical methods are used to sedate the pain. As TENS is a non-invasive method with no side effect, we seek to study it here in this paper. This is a clinical trial research conducted on 120 women aging 18 to 40 without any particular background disease with any parity who had a natural delivery in Taleghani Center. All the participants were chosen through a random selection procedure. In one group, TENS was placed on both sides of the back and around T10 to L1 and S2 to S4 half an hour, 1 hour and 6 hours after operation. The information correlated with two hours after delivery, while using TENS (the first and the sixth hour) and 6 hours after delivery was measured and recorded. The results showed no statistically significant difference between the average age of participants in the control and case groups. The average scale of pain within the first hour following the operation showed no statistically significant difference. However, the average scale of pain in the 2nd, 6th, and 12th hour following the operation exhibited a statistically significant difference between the two groups (P-value < 0.05). Considering the great advantages of TENS such as its safety and no side effects and toxicity, non-invasiveness and its simplicity, we may recommend TENS as an effective method to reduce natural delivery induced pain.
KEYWORDS: Electrical Stimulation; Pain; Natural delivery
Download this article as:| Copy the following to cite this article: Maktabi M, Nouruzi A, Farzinnia Z, Kamali A. Studying the Influence of Transcutaneous Electrical Nerve Stimulation (TENS) on Reducing the Post-natural Delivery Pain During Breastfeeding Period. Biosci Biotech Res Asia 2016;13(4). |
| Copy the following to cite this URL: Maktabi M, Nouruzi A, Farzinnia Z, Kamali A. Studying the Influence of Transcutaneous Electrical Nerve Stimulation (TENS) on Reducing the Post-natural Delivery Pain During Breastfeeding Period. Biosci Biotech Res Asia 2016;13(4). Available from: https://www.biotech-asia.org/?p=17389 |
Introduction
Pain is a really unpleasant feeling transmitted through the sensory neurons to brain. This signal indicates a real or potential damage caused to the body. However, pain is more than a physical feeling or sense. What’s more, understanding is the mental interpretation of discomfort. Interpreting the information is about the location, intensity and nature of it. Various conscious or unconscious responses to feelings and understandings including the emotional response are general concepts of pain (1). Birth pain is a set of regular uterine contractions whose intensity, frequency and length increase and result in natural vaginal child birth (2). Uterine contractions remain constant within few hours after child birth and various researches have pointed to the fact that post-child delivery contractions of uterine are much similar to the same contractions that give birth to neonatal (3). Labor pain is caused by uterine contractions and cervix dilatation transmitted through sympathetic nerves of visceral afferents stretching in spinal cord from T10 to L1. In further labor phases, the painful stimulus caused by pulling Perineum are transmitted through pudendal nerve and sacral nerves S2 to S4 (4). TENS (Transcutaneous electrical nerve stimulations) is one of the methods used to vanquish the pain in the injured parts of the patients. The electrode placed on the skin constantly stimulates the surface nerves and prevents transmission of pain signals (5). Various medical treatments are used to sedate the pain. As TENS is not invasive and has no side effects, we decided to study it. TENS carries out an electrical stimulation of nerves through skin in the form of an electrical current with low voltage in order to reduce the pain. This device consists of two electrodes connected to the skin in the area of pain or pressure. Then, a circuit of electrical impulses is created along the nerve fibers and the individual will feel less pain. We may set the device to various frequencies and wavelengths. TENS is used to reduce the pain in various diseases and various conditions. It is used in acute and chronic pains, muscular complications, joints, bones, arthritis, backache, neck ache, tendonitis or bursitis, cancer and child birth pains (4). As many as 7000 papers have been published on TENS and PUBMED and about 300 of them deal with the issues of delivery, post-delivery and breastfeeding period. Few researches are conducted in Iran concerning TENS in the process of child birth.
Material and Method
This is a single-blind clinical trial. 120 healthy women without any particular diseases aging 18 to 40 with any form of parity (primigravida or multigravida) who had a natural child birth in Taleghani Center were selected for our research. All the patients had taken TDS 250 mg Mefenamic acid and diclofenac suppository. A third person who knew nothing about the goal and purpose of research was charged with collecting data and analyzing the information. The participants were randomly divided into two groups and both groups were synchronized with one another in terms of parity and age. One group utilized TENS while the other did not. Painkilling through medicines was never stopped for any of the two groups (painkillers were used if VAS ≥ 5). TENS was placed on both sides of the back and around T10 to L1 and S2 to S4 half an hour, 1 hour and 6 hours after operation. The information correlated with two hours after delivery, while using TENS (the sixth hour) and 12 hours after delivery was measured and recorded. 4 pads were required for every individual and these pads were placed around T10 to L1 and S2 to S4. The size of the pads was 100*40. The frequency of device was set to 100 Hz. The device used in this research was ELLE TENS made by London based Body Clock Health Care Ltd with an output voltage of 0-110 mA. This company was represented by Tasnim Behboud Arman Co in Iran.
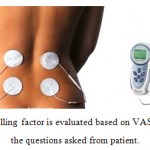 |
Figure 1 |
The pain killing factor is evaluated based on VAS criteria in the questions asked from patient.
| No pain | 0 |
| Little pain | 1 – 3 |
| Average pain | 4 – 6 |
| Severe pain | 7 – 10 |
 |
Figure 2 |
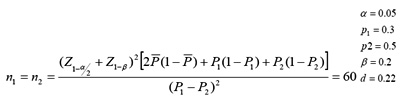
Those women having natural child delivery including those with primipara or multipara who had no background disease or their disease was controlled were included in the research, while those mothers who had an advanced or uncontrolled background disease or had no desire to take part in the research or were not interested in breastfeeding were excluded. If the selected individuals had no desire to continue the research or there was a problem placing the TENS, they would be excluded. The individuals were selected randomly based on the exclusion and inclusion criteria. Based on α = 0.05, the generalizable portion of 0.03 for population and according to previous researches, 60 participants were selected for each group. Overall, there were 120 participants in our research.
A questionnaire was prepared and the patients were asked about the effect of scale of pain and sense of comfort with TENS and their desire to repeat the procedure to reduce the pain. They were also asked to talk about the comfort of breastfeeding. After data collection was over, SPSS19 was used to analyze the data.
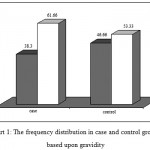 |
Figure 3: The frequency distribution in case and control groups based upon gravidity |
Inclusion criteria
all women aging 18-40 who have had a child delivery with no background disease or with a controlled background disease.
Exclusion criteria
an uncontrolled background disease, patient’s rejection, a skin disease where implanting the electrode is not possible.
Results
The following results were achieved while studying the effect of TENS on reducing post-child birth pain: there were 23 people (38.3%) with primipara and 37 people (61.66%) with multipara in the case group, while there were 28 people (46.66%) with primipara and 32 people (53.33%) with multipara in control group. As P-value ≥ 0.05, no statistically significant difference was observed between the two groups. The average age and standard deviation in control and case group were 32.1 ± 40.7 and 28.7 ± 9.4 respectively. As P-value ≥ 0.05, no statistically significant difference was observed between the two groups. On the other hand, the average and SD of scale of pain within the 1st hour in the case and control group were 9.03 ± 0.90 and 9.08 ± 0.96 respectively. As P-value ≥ 0.05, no statistically significant difference was observed between the two groups. However, a significant difference was observed between the average VAS between two groups within the 2nd, 6th and 12th hour (P ≤ 0.001) and VAS in the control group was significantly less than what was observed in TENS.
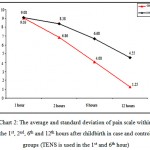 |
Figure 4: The average and standard deviation of pain scale within the 1st, 2nd, 6th and 12th hours after childbirth in case and control groups (TENS is used in the 1st and 6th hour)
|
Discussion
The present research was conducted to study the effect of TENS on pain reduction after natural child birth during the breastfeeding period. The average and standard deviation of pain scale in the first hour which coincided with using TENS exhibited no statistically significant difference between the case (TENS) and control groups (P ≤ 0.05). However, a significant difference was observed between the two groups within the 2nd, 6th and 12th hour after operation and the scale of pain was clearly much less in TENS group (P ≤ 0.001).
In a research conducted in the department of Gynecology and Physical Medicine in Afyonkarahisar Kocatepe (2014), it was shown that 2 groups of the total four groups who had taken TENS required a significantly less dose of painkiller after 8 hours. In the caesarean group, the group who had received TENS had significantly less problems. Our research also proved the effectiveness of TENS in reducing the post-natural childbirth pain which was in line with the results of the above said research. Another single blind study was also carried out by Physiotherapy Department of Sudan (2007) where the high to low frequency of pain decreased significantly among the 12 patients who had used TENS and these results are in line with the results achieved in our research. In another randomized clinical trial study conducted in the federal college of Alfenas (2014), TENS electrodes were placed on the T10_L10 and S2_S4 area of 32 multipara women after childbirth during breastfeeding period. These electrodes were then stimulated with a frequency of 100 Hz. This stimulation lasted 40 minutes and the pain caused by uterine contractions had significantly decreased in this group. The results of this study are also in line with our results. In another single-blind, randomized clinical trial conducted in Kerman University of Medical Sciences (2014), 150 women undergoing caesarean were studied and it was shown that the TENS group experienced the highest rate of pain reduction after operation. The TENS group was also reported to experience less pain in our group rendering our results in line with the results obtained in that research. In another study conducted in Shahid Akbar Abadi Hospital of Tehran (2008) to compare the effect of combining promethazine and pethidine with TENS in reducing childbirth pains in the active phase of childbirth. The level of pain in 3-4 cm dilatation was significantly less in TENS group. However, no significant difference was observed between the two groups in 6-7 cm dilatation and full dilatation. The number of contractions in TENS group in full dilatation was more and there was no difference in the time of childbirth. The above-said research has studied the influence of TENS on the progress of labor, but our research is focused on studying the effect of TENS in reducing post-childbirth pain. The above-said research is not in line with ours as we have compared it against the therapeutic effect of mixture of promethazine and pethidine. However, our research has studied the effect of TENS in both groups without interference from any additional drugs. In a clinical trial research carried out in the women surgical ward of Afzalipour Hospital of Kerman (2006), it was shown that the electrical effect of nerve through skin was really efficient in reducing the caesarean-induced pain. The results of that research are in line with those of the current study. A double-blind research carried out on 64 patients who had undergone caesarean operation in Imam Sajad (PBUH) Hospital of Yasuj (2002) showed that the level of pain and dose of the drug used by the case group was significantly less. This is in line with the results of our research. In 2001, research was conducted in Ardebil to study the effect of TENS on childbirth pains among those patients resorting to Alavi Hospital. A high frequency TENS machine with low wavelength was utilized and they arrived at the conclusion that TENS was capable of reducing the childbirth pain significantly and shorten the length of uterine contractions. But TENS was not capable of reducing uterine contractions and their power. The more you use TENS, the more effective will the machine be. Although we had not used TENS within the 2nd and 12th hours in our research, the long-term effect of using TENS on patients was quite clear. We may conclude that this research was in line with ours in terms of pain reduction and long-term influence of TENS. In single-blind research conducted in Medical Sciences University of Sabzevar (2000), 120 primigravida mothers aging 16 to 35 with a pregnancy length of 38 to 42 weeks who had resorted to maternity hospitals of Mashhad were studied. The first step of research pointed to pain reduction and shortening of active phase length. It had no influence on the scale of pain in the second phase childbirth but the progress had grown shorter. TENS was reported to influence the post-childbirth pain in our research and this difference is justifiable as the current research is conducted in the labor progress.
Table 1: Descriptive statistics of age indicator in case and control groups
| Group | Number | Average ± SD | P-value | |
| Age | Control
Case |
60
60 |
32.1 ± 40.7
28.7 ± 9.4 |
0.622
Nonsignificant |
Conclusion
Based on these results, we may conclude that patients will feel less pain while using TENS compared to other states. This influence continued in post-TENS application period, i.e. within the 1st and 12th hours when TENS was not used, there was a significant reduction of pain. Thus, TENS is really effective in reducing the natural childbirth-induced pain. Thus, TENS may be recommended as a really useful method to reduce natural childbirth-induced pain. Keeping in mind various advantages of TENS (e.g. safety, no side effects or toxicity, non-invasiveness, simple and easy application), it is recommended to expand and develop the utilization of this method. It is therefore recommended to carry out similar researches with a greater number of samples.
Reference
- Olsén MF, Elden H, Janson ED, Lilja H, Stener-Victorin E. A comparison of high- versus low-intensity, high-frequency transcutaneous electric nerve stimulation for painful postpartum uterine contractions. Acta Obstet Gynecol Scand. 2007;86(3):310-4. PubMed PMID: 17364305
CrossRef - Wei L, Wang H, Han Y, Li C. Clinical observation on the effects of electroacupuncture at Shaoze (SI 1) in 46 cases of postpartum insufficient lactation. J Tradit Chin Med. 2008 Sep;28(3):168-72. PubMed PMID: 19004195.
- Dowswell T, Bedwell C, Lavender T, Neilson JP. Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD007214.
- Kayman-Kose S, Arioz DT, Toktas H, Koken G, Kanat-Pektas M, Kose M, Yilmazer M. Transcutaneous electrical nerve stimulation (TENS) for pain control after vaginal delivery and cesarean section. J Matern Fetal Neonatal Med. 2014 Oct;27(15):1572-5.
CrossRef - De Sousa L, Gomes-Sponholz FA, Nakano AM. Transcutaneous electrical nerve stimulation for the relief of post-partum uterine contraction pain during breast-feeding: a randomized clinical trial. J Obstet Gynaecol Res. 2014 May;40(5):1317-23
CrossRef - F. Gary Cunningham Kenneth J. Leveno Steven L. Bloom Catherine Y. Spong Jodi S. Dashe.Barbara L. Hoffman.Brian M. Casey.Jeanne S. Sheffield.Assessment .section 24. chapter 7. williams obstetric and gynecology 24th Edition
- Ali Mohamadian M, Shariat M, Mahmoudi M, Ramazanzadeh F. The Influence of Maternal Request on the Elective Cesarean Section Rate in Maternity Hospitals in Tehran, Iran. Payesh. 2003; 2(2):133-139.
- Bedwell C, Dowswell T, Neilson JP and Lavender T. The use of transcutaneous electrical nerve stimulation (TENS) for pain relief in labor: A review of the evidence. Midwifery 2010; 1: 65-69.
- Beischer N, Mackay E. Obstetrics and newborn. 3rd ed. New York: W.B Sanundres; 1995: 125-9.
- Bragg F, Cromwell D A, Edozien L C, GurolUrganci I, Mahmood T A, Templeton A. Variation in rates of caesarean section among English NHS trusts after accounting for maternal and clinical risk: cross sectional study. Brit Med J 2010; 341(5065): 1-8.
CrossRef - Hamilton BE, Martin JA, Ventura SJ. Births: preliminary data for 2010. Natl Vital Stat Rep 2011;60(2):1-25.
- Lenehan GP. On alternative theme issues. J Emerg Nurs. 1998;24(6):476-7.
CrossRef - Nesionpour S. Pain. 1st . Tehran. Teimourzadeh Company. 2004; pp: 319-320.
- Potter PA, Perry AG. Basic nursing: Theory and practice. 13th . ST Louis. Mosby Company. 2003; p:742.
- Ronald S. Gibbs; Beth Y.Karlan ; Arthur F.Haney ; Ingrid Nygaard. Danforth’s Obstetrics and Gynecology.Lippincott Williams & Wilkins , 10th ed, 2008.
- Torloni M R, Daher S, Betrán A P, Widmer M, Montilla P, Souza J P. Portrayal of caesarean section in Brazilian women’s magazines: a 20-year review. Brit Med J 2011; 342(276): 1-7.
CrossRef - Zanouze, F.; Hashemi Jam, M.S.; Comparing the effect of TENS with mixture of pethidine-promethazine on reducing the childbirth pains in the active phase of child delivery, Iran Medical Scinces University Magazine, 15th period, Nos. 60-61, autumn of 2008.
- Mazhari, F.; Rezaie, H.; Alizadeh, S.; Studying the effect of TENS on post-caesarean pain control, Jahad Daneshgahi Scientific Information Base, 2007.
- Rostaminezhad, A.; Khosravi, A.; Karimi, Z.; Mohamad Hosseini, S.; Sheykhi, F.; Bahadori, L.; The influence of TENS on controlling post-caesarean pain, Jahad Daneshgahi Scientific Information Base, 2007.
- Ebrahimi Houshiyar, A.; Hossein Rezaei, H.; Jahani, Y.; Kazemi, M.; Monfared, Sh.; Comparing two aromatherapy methods using lavender’s essence and TENS in reducing post-caesarean pain, 18th period, No. 146, 6-12.

This work is licensed under a Creative Commons Attribution 4.0 International License.



