

How to Cite | Publication History | PlumX Article Matrix
Adil A. Abdul Razaq1, Chateen I. Ali Pambuk1 and Yahya J. Salman2
1College of Dentistry, Tikrit University , Iraq.
2Department of Microbiol., Kirkuk Faculty of Medicine , Iraq.
Corresponding Author E-mail: chatin2@yahoo.com
DOI : http://dx.doi.org/10.13005/bbra/2555

ABSTRACT: In recent works Helicobacter pylori (H. pylori) become a significant criteria and essential diagnostic tool for studying the etiology of gastro-intestinal tract disorders (GITDs), for this purpose a total of stool samples were collected from 266 patients from both gender ,they were aging from below one year to over than 70 years. Their compliance with epi-gastric pain, diarrhea weigh loose and other disorders. Types of GITDS were detected and classified by the gastro-enterologists in two main Hospitals and from patients attending Private clinics and medical labs in Kirkuk city. H. pylori was detected form stool samples by using rapid lateral immune-chromatography assay (RLICA). GITDs involve, H. pylori positive distributed in 132 (49.62%), followed by 74 (27.81 % ), 59(22.18 %), 7(2.63 %), 3(1.12%) and 2(0.75 %) for irritable bowel diseases, inflammatory bowel diseases, peptic ulcer, ulcerative colitis and duodenal ulcers diseases respectively. Whereas 171, (64.28%) were positive for parasitic infection, P<0.05 .Moreover other 48, (18.04 %) stool samples were non-identified it's about from the described diseases. A total of132 (49.62 %) of H. pylori positive samples were distributed in 46(38.84 %) samples for IBD versus to 41(31.81 %) for IBS and 33(25%) were positive for parasitic infections, p <0.05. According to age; highest rate 10 (55.55 %) of H. pylori was recorded among patients aging from 61 to 70 years, whom they have IBD. Whereas 7 (70 %) have IBS within age group from 41 to 50 years, P <0.05. It can be that H. pylori participate with high rate in GITDs patients particularly IBD elderly patients.
KEYWORDS: GITDs H.IBD; IBS; pylori; Peptic ulcer.
Download this article as:| Copy the following to cite this article: Razaq A. A. A, Pambuk C. I. A, Salman Y. J. Role of Helicobacter Pylori in Gastro-Intestinal Tract Disorders (Gitds) Among Patients in Kirkuk City, Iraq. Biosci Biotech Res Asia 2017;14(3). |
| Copy the following to cite this URL: Razaq A. A. A, Pambuk C. I. A, Salman Y. J. Role of Helicobacter Pylori in Gastro-Intestinal Tract Disorders (Gitds) Among Patients in Kirkuk City, Iraq. Biosci Biotech Res Asia 2017;14(3). Available from: https://www.biotech-asia.org/?p=27159 |
Introduction
Gastrointestinal tract (GIT) is vital system in the body of human being, is an organ system within human and other animals which takes the food and digests it to extract and absorb energy and nutrients and expects the remaining waste as feces and urine.1 Maintaining GIT healthy from any infectious agents give raises healthy body. The more famous mysteries to this system are factorial involving; inflammation that can be seen as inflammatory bowel disease (IBD) either organic or inorganic types.2 Additionally irritable bowel syndrome (IBS) that is resemble somewhat to IBD also considered as the second health problem to GIT. 3
Moreover since about 30 years Helicobacter pylori(H.pylori ) ,which is gram negative , flagellated , spiral bacterium that colonizes the gastric mucosa in humans, causing chronic active gastritis type B and peptic ulcer disease that has serious impact on the host.4 Both microorganisms if aren’t treated properly and eradicated from the GIT; they may lead in to ulcerative colitis induced by Entamoeba histolytica and several organs in extra-intestine may involve such as liver ,lungs and brain producing abscess.5 While Helicobacter pylori un proper management mostly progress in to stomach cancer produced by different three virulent factors such as cytotoxic associate gene factor (Cagf).6
The etiology of GIT particularly IBD may extend to involve Crohn agents such as that genetic susceptibility, environmental factors and body immune responses. The picture of this disease characterized by ulceration of any part of GIT particularly the colon which is mostly associated with fistula mascularis and formation between colon and vagina .Also it may extend to and reaches to perineum. 7 The adverse actions of IBD and IBS mostly characterized by severe diarrhea either liquid diarrhea in case IBS and bloody mucoid diarrhea in case of IBD , some alteration with constipation, nausea , weight loss , fever ,loss of appetite ,fatigue and with time anal bleeding.8 Helicobacter pylori It is helical or spiral in shape from which its name was derived, its gram –negative bacteria, microaerophilic {it requires oxygen but at lower levels than those contained in the atmosphere}.Its oxidase, catalase positive.9 Motile bacterium with5-7 unipolar flagella , with its flagella and its spiral shape this bacteria can drills in to mucus layer of the stomach .Its produces adhesins which bind to membrane- associated lipids and carbohydrates and helps the bacteria to adhesion to epithelial cells.10 It’s the only known microorganisms that can thrive in the highly acidic environment of the stomach.11
This bacteria is safely ensconced in the mucus and its able to fight the stomach acid that does reach it with an enzyme it possessed called (Urease), that converts the urea of which there is an abundant supply in the stomach from saliva and gastric juices , in to bicarbonate and ammonia which are strong bases , this creates a cloud of acid that neutralizing chemicals around the bacteria and protecting it from the acid in the stomach.12 For the importance of H. pylori that mentioned in the above the current study was conducted to show role of H. pylori in GITDs patients in Kirkuk city-Iraq for the first time in Iraq.
Material and Methods
From a period of 1st July 2016 to 31 March 2017 in Kirkuk city a total of 266 stool samples were collected from patients attends in to Azadi-teaching and Kirkuk general Hospitals , Private clinics and private medical labs. Males contribute 141 versus to 125 females; their ages ranged from below one year to over than 70 years. From each patient complete information were arranged in special questionnaire. Stool samples were distributed in to 3 portions in sterile cup fitted tight; first part directed transferred in to refrigerator for calprotectin assessement, second portion directly processed for H. pylori detection in stool samples using RLICA kit. Whereas for third portion was preserved with sufficient amount of 2.5 % of potassium dichromate and left for parasites detection.
Quantitative fecal calprotectin(FC) ELISA test was performed for each stool specimen for detecting FC .This ELISA kit was purchased from Epitope Diagnostic Int (EDI) company-USA. This ELISA is designed, developed and produced for the quantitative measurement of human calprotectin in stool samples. The assay utilizes the two-site (Sandwich) technique with two selected antibodies that bind to different epitopes of human calprotectin.
The second fraction was searched for stool antigen test for H. pylori using RLICA (cassette test). The test briefly is simple modified ELISA for detecting Helicobacter pylori in the stool as antigen with immobilized monoclonal antibodies bound on the chromatography pad inside the special cassette containing enzymatic conjugate (HRP) and Substrate as ( TMB) ., the method briefly started by transporting small portion of stool sample in the small container containing buffer , mixed thoroughly then about 2 drops ( 80 microliters ) were inserted in to specific hole. Before 10 minutes the pink to red bands (control and test) mean positive for H.pylori while appearing only control band and means negative result. This method was done according to the leaflet of Bio-zek company-Netherland.
Direct microscopy procedures as double wet preparations of 0.9 % of NaCl and 1 % of Lugols iodine were done according to (WHO, 2003) for detecting parasitic stages from third portion of collected stool samples.
Statistical Analysis
All obtained data from stool samples processing were arranged in tables and figures and were checked statistically by using chi-square test and t-student test as significant when the differences between two analyzed parameters were at P<0.05.
Results
From examining a total of 266 of stool samples , the following results were recorded in Figure – 1 ,is exerting patients distributions in the current study as follows ; a total 132 (49.62%) positive results of H. pylori antigen , followed by a total of 74 (27.81 % ) for irritable bowel diseases, , 59 (22.18 %) inflammatory bowel diseases , 51(19.17 %) positive results for Calprotectin antibody and 7(2.63%),3 (1.12%), 2 (0.75%) patients with peptic ulcer, ulcerative colitis and duodenal ulcers diseases respectively . Whereas a total of 171, (64.28%) of positive results were for parasitic infection .Moreover other 48, (18.04 %) stool samples were non-identified it’s about from the described diseases.
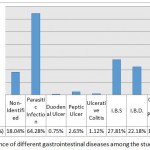 |
Figure 1: The Prevalence of different gastrointestinal diseases among the study group in Kirkuk city. |
Helicobacter pylori antigen. On the other hand according to types of GITDs the following results were obtained: 46 (34.84 % ) were positive Helicobacter pylori antigen in inflammatory bowel diseases versus 13 (9.70 % ) of negative Helicobacter pylori antigen in inflammatory bowel diseases, followed by 42 (31.81%) of positive Helicobacter pylori antigen among irritable bowel diseases, contrary to 32 (23.88% ) of negative Helicobacter pylori antigen in irritable bowel diseases. While all cases of Ulcerative colitis show positivity for Helicobacter pylori antigen, the rate was (2.27%) . For peptic ulcers only 6 (4.54%) stool samples were positive for Helicobacter pylori antigen compare to one sample with rate of (0.74 %) was negative Helicobacter pylori antigen. Also all tow cases as they have duodenal ulcer exert positivity (1.51%) for Helicobacter pylori antigen, followed by 33(25%) of positive Helicobacter pylori antigen recorded in parasitic infections Whereas 134 (50.37 % ) stool samples were negative for H. pylori
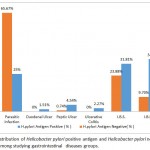 |
Figure 2: The distribution of Helicobacter pylori positive antigen and Helicobacter pylori negative antigen cases among studying gastrointestinal diseases groups. |
Table-1 showing the distribution of Helicobacter pylori according to types of the diagnosed diseases, from a total of 266 examined patients only 132(49.62 %) were positive for Helicobacter pylori. Frequencies of positivity was distributed in to 53(19.92 % ) among the specimens belongs to IBD compare to 49(18.42 %) among IBS statistically the relationship was not significant ,P>0.05.Also in the same table both types of the diseases were not recorded among patients aging below 10 years . High rate of Helicobacter pylori 70% was recorded among IBS aging from 41 to 50 years versus to 28.57% among patient aging from 31 to 40 years suffering from IBS ,P<0.05.Contrary to those among IBS patients there distribution for Helicobacter pylori positivity was not significant ,p>0.05.
Table 1: Frequencies of Helicobacter pylori antigen positive and antigen negative in relation to patients ages.
| Ages/years | Total Examined No (%) | H.pylori Stool+serum Positive No(%) | H.pylori Stool +ve No(%) | H.pylori Serum +ve No.(%) | Total H.pylori Positive No (%) | H.pylori Negative N (%) |
| 1—10 | 27( 10.15) | 11(40.74) | 2(7.40) | 10(37.03) | 23(85.18) | 4(14.82) |
| 11—20 | 42(15.85) | 17(40.47) | 3(7.10) | 11(26.19) | 31(73.81) | 11(26.19) |
| 21—30 | 41(15.39) | 12(29.26) | 1(2.43) | 12(29.26) | 25(60.97) | 16(39.03) |
| 31—40 | 56(21.05) | 30(53.57) | 2(3.57) | 7(12.50) | 39(69.54) | 17(30.36) |
| 41—50 | 50(18.77) | 22(44.00) | 2(4.00) | 11(22.00) | 35(70.00) | 15(30.00) |
| 51—60 | 32(12/03) | 14(43.75) | 1(3.12) | 9(28.15) | 24(75.00) | 8(25.00) |
| 61—-70 | 18(6.75) | 13(72.22) | 2(11.11) | 2(11.11) | 17(94.44) | 1(5.56) |
| Total | 266 | 119(44.73) | 13(4.88) | 62(23.30) | 194(72.94) | 72(27.06) |
Total number examined samples were 266 for each of stool and serum.
Discussion
This current study show the relationships between Helicobacter pylori positive and Helicobacter pylori negative antigen among gastrointestinal studying diseases, the rate of patients classified as idiopathic Helicobacter pylori positive antigen results among 266 patients were 49.62% , and Helicobacter pylori negative antigen results was 50.37 % , the result of the present study contraindicated with a study conducted by Bashdar M. et al. positive rate was 55.8%, negative rate was 44.2 % in Erbil city and by Abdelrazk et al.13 positive rate was 54.5 % , and negative rate was 45.5 % in Egypt .And in the current study the rate of positive Helicobacter pylori antigen in inflammatory bowel diseases was 34.84 % , were the rate of negative Helicobacter pylori was 9.70 % ,this results of the present study agrees with Haider et al.15 that were results ratio was 22.86 % , 77.14 % in Baghdad . And in the current study the rate of positive Helicobacter pylori antigen in irritable bowel syndrome was 31.81 % , and negative Helicobacter pylori antigen ratio was 23.88 % , the result of the present study contraindicated with a study conducted by Feng et al.16 that were results was 41.04 % positive and 58.96 % negative results . And in the current study the rate of ulcerative colitis was 2.27 % from all cases positive Helicobacter pylori , and the result of the present study agrees with Xi Jin et al.17 that the rate was 30.5 % in china. . And in the current study the rate of peptic ulcer diseases was 4.54 % in positive Helicobacter pylori antigen and 0.74 in negative Helicobacter pylori, and this result of the present study agrees with Mohammad et al.18 that was the ratio in positive Helicobacter pylori antigen was 59 % and in negative was 41% in sulaminai city. In present study the rate of duodenal ulcer was 1.51 % , and this result in the present study contraindicated with a study conducted by Ruba et al.19 in Jorden. And in the current study the ratio of parasitic infection in positive Helicobacter pylori antigen was 25 % , and 65.67 % in negative Helicobacter pylori antigen, this result of the present study agrees with Hossein et al.20 that were ratio was 43 % in positive Helicobacter pylori antigen , and 57 % in negative Helicobacter pylori antigen.
This current study show that the relationship between Helicobacter pylori positive antigen and irritable bowel syndrome and inflammatory bowel diseases according to patients ages , the distribution of Helicobacter pylori according to types of the diagnosed diseases, from a total of 266 examined patients only 132(49.62 %) were positive for Helicobacter pylori. Frequencies of positivity was distributed in to 53(19.92 % ) among the specimens belongs to IBD compare to 49(18.42 %) among IBS statistically the relationship was not significant ,P>0.05.Also in the same table both types of the diseases were not recorded among patients aging below 10 years . High rate of Helicobacter pylori 70% was recorded among IBS aging from 41 to 50 years versus to 28.57% among patient aging from 31 to 40 years suffering from IBS ,P<0.05.Contrary to those among IBS patients there distribution for Helicobacter pylori positivity was not significant ,p>0.05.The total positive rate of irritable bowel syndrome was 18.42 %, the result of the present study contraindicated with a study conducted by Abdelrazak Mansour et.al.21
Also in the same present study the high rate of inflammatory bowel diseases of Helicobacter pylori positive antigen 100 % between two age group between 11-20 years and 61-70 years old, and the lower rate 66.67% was between 21-30 years old patients. The total positive rate of inflammatory bowel disease was 19.92 % , the result of the present study agrees with T. Rokkes et.al.22
Acknowledgements
This research was supported by research grants of post graduate studies from The Ministry of higher education and scientific Research of Iraqi Government, Which provided by the College of Science Tikrit University.
Conflict of Interests
No conflict of interest in this current study
References
- Helander H. F., Fändriks L. Surface area of the digestive tract – revisited. Scandinavian Journal of Gastroenterology. 2014;49(6):681–689.
CrossRef - Fengming Y., Jianbing W. Biomarkers of inflammatory bowel disease.Dis.Markers. 2014:276-282.
CrossRef - Lovell R. M., Ford A. C. Global prevalence of and risk factors for irritable bowel syndrome a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712-721.
CrossRef - Cid T. P., Fernández M. C., Martínez S. B., Jones N. L. Pathogenesis of Helicobacter pylori Infection. Helicobacter . 2013;18:12-17 .
CrossRef - Ravdin J. I . Amebiasis clinic. Infected diseases . 2013;20:1453-1566.
CrossRef - Yamaoka Y. Mechanisms of disease: Helicobacter pylori virulence factors. Nat Rev .Gastroenterol . Hepatol. 2014;11(15):629-641.
- Eglinton T. W., Roberts R., Pearson J., et al. Clinical and genetic risk factors for perianal Crohn’s disease in a population-based cohort. Am J Gastroenterology. 2012;107:589–596.
CrossRef - Castaño-Milla C., Chaparro M., Gisbert J. P. Systematic review with meta-analysis: the declining risk of colorectal cancer in ulcerative colitis. Aliment Pharmacology.Ther. 2014;39:645–659.
CrossRef - Kuo C. H.,Chen Y. H., Goh K. L., Chang L. L. Helicobacter pylori and Systemic Disease. Gastroenterol. Res. Pract. 2014:358–494.
- Monzón H.,Forné M., Esteve M., Rosinach M.,Loras C., Espinós J. C., Viver J. M., Salas A., Fernández-Bañares F. Helicobacter pylori infection as a cause of iron deficiency anaemia of unknown origin. World J. Gastroenterol. 2015;21:4166–4171.
- Bravo L. E., Realpe J. L., Campo C.,Mera R., Correa P. Effects of acid suppression and bismuth medications on the performance of diagnostic tests for Helicobacter pylori Am. J Gastroenterol. 2012;107:2380–2383.
- Atli T., Sahin S., Arslan B. U.,Varli M.,Yalcin A. E., Aras S. Comparison of the C14 urea breath test and histopathology in the diagnosis of Helicobacter pylori in the elderly. J. Pak. Med. Assoc . 2012;62:1061–1065.
- Abdelrazak M. A., Walid F. E. Potential complication of Helicobacter pylori infection in children of non urban community. 2015;3(2):e23510.
- Bashdar M., Saleem S. Q. et al. The prevalence of Helicobacter pylori among university students in Iraq. 2013;0974-5645.
- Faizal H. G., Abdulmohaymen N. M., Jawad R. H . The association of ATG16L. Thr300Ala Allelic Variant with Helicobacter pylori infection among IBD patients. 2015;4(11):650-658.
- Xiong F., Xiong M., Ma Z., et al . Lack of association found between Helicobacter pylori infection and diarrhea predominant IBS. 2016;7:3059201.
- Jin X., Yi-Peng C., Shao-nua C . Association between Helicobacter pylori infection and ulcerative colitis case control study from China . 2013;10(11):1479-1484.
- Mohammad O. M. Correlation of endoscopic findings with various Helicobacter pylori test among dyspeptic patients .2014;5:1180-1188.
- Ruba S. Abu-sbeih., Azmi D. H., Dhia S., et al . Isolation and detection of Helicobacter pylori from patients suffering from peptic ulcer using biochemical tests and molecular techniques . 2014;10(1):58-68.
- Kazemian H., Heidari H., Kardan J. Y . Relationship between Helicobacter pylori infection and parasitic infection in patients in llam. 2016;2:15-17.
- Mansour A., Ali M., Abdelraheem M. M. Irritable bowel syndrome in children . 2014;1:2.
- Rokkes T.,Gisbert J. P and Comerain Y. N. The association between Helicobacter pylori infection and irritable bowel syndrome based on meta- analysis . 2015;3(6):539-550

This work is licensed under a Creative Commons Attribution 4.0 International License.



