

How to Cite | Publication History | PlumX Article Matrix
Epidemiology and Risk Factor of Lung Cancer in Morocco
Amal Haimer*1 , Souad Belamalem1, Faouzi Habib2, Abdelrhani Mokhtari1 , Abdelmajid Soulaymani1and Hinde Hami1
, Souad Belamalem1, Faouzi Habib2, Abdelrhani Mokhtari1 , Abdelmajid Soulaymani1and Hinde Hami1
1Laboratory of Genetics and Biometry, Faculty of Science, Ibn Tofail University, Kenitra, Morocco.
2Al-Azhar Oncology Center, Rabat, Morocco.
Corresponding Author E-mail: amal.haimer@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/2720

ABSTRACT: The aim of this study is to describe the epidemiological characteristics of lung cancer in Morocco. This is a descriptive retrospective analysis of lung cancer cases, diagnosed and treated at Al Azhar Oncology Center in Rabat over a period of 11 years, between 2005 and 2015. Among the 615 cases that were diagnosed with lung cancer at Al Azhar Oncology Center, 85.85% were male and 14.15% female, the mean age of men with lung cancer was 59.8 ± 11.2 years while that of women was 58.6 ± 12 years. During the study period, there were 129 deaths from this type of cancer, of which 89.9% were men and 10.08% were women. The maximum frequency of death was observed in patients aged between 40 and 60 years with 54.80%. Of all diagnosed cases, 2.40% were diagnosed with metastatic disease. The majority of patients received chemotherapy treatment with 47%, followed by patients who received radiotherapy with 42.3%. On the other hand, the study shows that there is an association between the risk of progression to death and smoking. Lung cancer is dreaded especially in the male population with a high number of cases and lethality as well as a poor prognosis.
KEYWORDS: Epidemiological Profile; Lung Cancer; Retrospective Study
Download this article as:| Copy the following to cite this article: Haimer A, Belamalem S, Habib F, Mokhtari A, Soulaymani A, Hami H. Epidemiology and Risk Factor of Lung Cancer in Morocco. Biosci Biotech Res Asia 2019;16(1). |
| Copy the following to cite this URL: Haimer A, Belamalem S, Habib F, Mokhtari A, Soulaymani A, Hami H. Epidemiology and Risk Factor of Lung Cancer in Morocco. Biosci Biotech Res Asia 2019;16(1). Available from: https://bit.ly/2WzO1uF |
Introduction
Lung cancer is the most commonly diagnosed cancer in the world (with 1.8 million cases, 13% of the total). it is one of the most common causes of cancer deaths (1.6 million deaths, 19.4% of the total).1
Pulmonary cancer has become the most deadly cancer as much for women as for men.2 Despite improvements in diagnostic and therapeutic methods, overall survival has only increased from 9% to 14% in the last 20 years. However, the survival of very early stages (be stage 1) is higher (60 to 70%).3
In France lung cancer is the leading cause of death from cancer, it counts for 20.1% of all cancer deaths. It is the first cause of death for men (be 25% of all male deaths due to cancer), and the second cause for women (nearly 14% of all female deaths from cancer).4
In Canada, lung cancer is the most commonly diagnosed form of cancer (14% of all new cancer cases and 25% of all cancer deaths).5
In Morocco, lung cancer is the most common cancer for men, be 3391 cases (13.3%) and is also the leading cause of death with 3157 cases (12.5%).6
The aim of this study is to describe the epidemiological characteristics of lung cancer in Morocco.
Material and Methods
This is a retrospective epidemiological study that took place in Al Azhar Oncology Center over a period of 11 years, from January 2005 until December 2015.This center was founded in July 1994, it includes several units: chemotherapy, brachytherapy, surgery, ira-therapy and bone marrow transplant. A record is created for each patient and contains the location of the tumor, its nature, the protocol and the treatment monitoring. The variables we looked at in our study were sex, age onset of treatment, the evolution (death or non-death), as well as the date and age of death. It should be noted that patients whose deaths are not reported in the records may be either alive or lost to follow-up.
In this study, the indicator in Potential Years of Lost Lives was calculated. PYLL is a measure of the impact of illnesses and/or health problems in a society, showing losses which are mainly due to the death of young or premature persons.7
PYLL is the number of years that a subject dies prematurely before an age limit. The choice of the age limit at 65 corresponds to the threshold used by the WHO for international comparisons. Therefore, the calculation of PYLL is excluded8:
-All deaths occurring after the age of 65.
-infant deaths of less than one year because they are due to specific causes and often have a different etiology than deaths at a later age.
(id): is the number of the deaths in each age group
(ai): center of age class I
L: the upper age limit of the study
Results
A total of 615 lung cancer cases were collected during the study period, representing 7.76% of all cancer cases collected. Among lung cancer cases, 85.85% (528 cases) of males and 14.15% (87 cases) of females with a sex ratio of 6.06 (χ²=0.81; p=0.34).The average age of diagnosis of lung cancer for men was 58.6/// 11.2 years ( 4-94 years) and for women the average age was 58.6///12.4 years (81-83). The number of lung cancer death was 129, including 116 men (89.92%) and 13 women (10.08%). The sex ratio of lung cancer mortality was 8.92 in favor of men (P =0.001).
Figure 1 shows the annual distribution of the number of lung cancer identified and the annual evolution of deaths during the period going from 2005 and 2015. According to the results of this figure, there is a gradual increase in the number of cases; this increase is accentuated between 2007 and 2009 (from 46 cases to 90 cases). For the evolution of patients there are 129 deaths detected during the period from 2005 to 2015. The date of death was reported in 87 files only. The annual number of deaths peaks in 2010 with 15 cases (17.2%),then decrease in 2012 to a value of 6 cases (6.9%) and then increased considerably to 13 cases in 2013, to decrease in 2016 to a minimum value of 1.1% ( 1 case ).
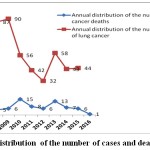 |
Figure 1: Annual distribution of the number of cases and deaths of lung cancer.
|
On the other hand, the distribution of the studied cases of pulmonary cancer according to the source is represented on figure 2. According to our results, the majority of patients are from the Rabat-Sale-Kenitra region with 279 cases (2.6%), followed by that of Tangier-Tetouan-Al Hoceima with 74 cases (13.7%) followed by Fez-Meknes with 57 cases (10.5%).
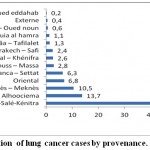 |
Figure 2: Distribution of lung cancer cases by provennace.
|
Table 1 shows the distribution of the number of cases of lung cancers recorded at the level of the center studied according to the WHO age groups. It can be seen that the age group (40-60) years old is the most affected, with 297 cases (50.3% of lung cancers) followed by the age group ≥ 60 which represents 47.1% of these cancers with 278 cases, then the class (30-40 years) with 11 cases (1.9% of lung cancers). Respecting the age groups distribution of lung cancer deaths, Table 1 shows that the age group (40-60) years has the highest frequency of death with 68 deaths (54.8%) while that class ≥ 60 comes second with 53 deaths (42.7%), followed by the class (30-40) years with 3 deaths (2.4%).
Table 1: the distribution of deaths by age group.
| Age classes (years) | Number of cases (%) | Number of deaths (%) |
| 15< | 2 (0,3%) | – |
| 20-30 | 2 (0,3%) | – |
| 30-40 | 11 (1,9%) | 3 (2,4%) |
| 40-60 | 297 (50,3%) | 68 (54 ,8%) |
| ≥ 60 | 22 (47,1%) | 53 (42,7%) |
| Total | 590(100 %) | 124 (100 %) |
Potential Years of Lost Lives were derived from the number of deaths in de age group included between 0 to 94 years, compared to the general population under 65 years of age. So the PYLL is 3.42 per 10 000 inhabitants for all victims who have suffered this pathology. Lung cancer is an influential factor in the causes of premature death, which represents 1156 potential years of lost lives.
Table 2: Potential Years of Lost Lives.
| Age class | Deaths | PYLL |
| 15>years | – | – |
| 20-30years | – | – |
| 30-40years | 3 | 90 |
| 40-60years | 68 | 1020 |
| 60-64 years | 19 | 46 |
| Total (2005-2015) | 1156 |
The distribution of the studied cases of lung cancer in accordance with the type of treatment is shown in table 3. The majority of patients received chemotherapy treatment with 47% (291 cases), followed by patients who received radiotherapy treatment with 42.3% (260 cases), then those who received targeted biotherapy with 21.76% (71 cases).
Table 3: the distribution of patients by type of treatment.
| Type of treatment | n (%) |
| Chemotherapy | 291 (47 %) |
| Radiotherapy | 260 (42,3 %) |
| Targeted biotherapy | 71 (11,5 %) |
| Corticoteroid therapy | 40 (6,5 %) |
| Hormonal therapy | 6 (1 %) |
| surgery | 1 (0,2 %) |
| Total | 669(100%) |
According to our results, 29.9% (n=18) of patients are smokers, 6.1% (n=38) have antecedents and 2.5% (n=18) have a metastatic cancer.
Table 4 presents the results of the risk factors that influence the evolution of patients. This table shows that there is no significant association between the evolution to death and sex, the same for age classes and the patients’ antecedents. However smoking is a risk factor where the odds ratio value is 1.15 at 95% CI is (1.15-2.51).
Table 4: Risk factors that influence the evolution of patients.
| Variables | Healing | Death | p | RR | IC 95 % | |
| Male | 412 | 116 | ||||
| Gender | 0,85 | 1,60 | 0,85-2,99 | |||
| Female | 74 | 13 | ||||
| 15 < | 2 | 0 | 0,62 | 1,26 | 1,21-1,32 | |
| 20-30 | 2 | 0 | 0,62 | 1,26 | 1,21-1,32 | |
| Age class | 30-40 | 8 | 3 | 0,41 | 1,41 | 0,37-5,43 |
| 40-60 | 229 | 68 | 0,15 | 1,25 | 0,84-1,87 | |
| ≥ 60 | 225 | 53 | 0,15 | 0,80 | 0,80-1,2 | |
| Yes | 66 | 185 | ||||
| Smoking | 0,005 | 1,70 | 1,15-2,51 | |||
| No | 63 | 301 | ||||
| Yes | 139 | 48 | ||||
| Antécédent | 0,039 | 1,48 | 0,98-2,22 | |||
| No | 347 | 81 |
Discussion
In spite of some advances in treatment, lung cancer is a common disease with a heavy morbidity and mortality. It is currently one of the major public health problems, with a global incidence of 1.2 million new cases per year.9
Our study has collected 615 cases of lung cancer over 10 years, with an annual average of 61 ± 14 cases per year. The majority of cases are from Rabat-Sale-Kenitra region. This is due to the proximity of the diagnostic center. With regard to sex, we found that men are more affected than women and the sex ratio (M/F) was 6.06. This result is similar to the literature data.1,10 This high male risk is mainly due to the toxic habits that are in most cases related to smoking which is the major cause of this pathology.11
According to the International Agency for Research on Cancer (IARC) it was estimated that in populations with prolonged smoking, the risk of having lung cancer is more than 90%.12 Our results revealed that 29.9% of patients are smokers. Thus, the calculation of the Odds ratio found that smoking is a major risk factor for this type of cancer. This result is consistent with the literature data.13-14-15 Moreover, in other works, smokers are at 20 times more likely to develop lung cancer than non-smokers.16 In fact, the risk of lung cancer in smokers depends on different aspects of smoking behavior, including the duration of smoking, the amount of cigarettes smoked and its types as well as the type of inhalation. This average age of lung cancer diagnosis for men was 59.8 ± 11.2 years and 58.6 ± 12.4 years for women. This average is discordant with the result of the literature data.17-10 The 40-60 age groups were the largest with a frequency of 50.3%. This result is similar to the literature data.18 The treatment of lung cancer depends on its extension. In our study, 47% of cases received chemotherapy. In other publications, radiotherapy is the most frequently used in 29% of cases.19
Conclusion
On the one hand, a good knowledge of the epidemiological and therapeutic aspects of lung cancer is essential for an early diagnosis and an adequate management. On the other hand, and considering the undeniable correlation smoking and lung cancer, it is necessary to intensify anti-smoking campaigns.
Acknowledgments
The authors are pleased to acknowledge to the entire research team of the Genetics and Biometry Laboratory at Ibn Tofail University.
Conflict of Interest
There is no conflicts of interest.
Funding Source
This work is part of the” PPR-B-Moukhtari-FS-ITU-Kénitra”.
References
- Torre L. A., Bray F., Siegel R. L., Ferlay J., Lortet-Tieulent J.,et Jemal A. 2015). Global Cancer Statistics, 2012. CA: un. journal sur le cancer pour les cliniciens. 2015;65(2):87-108.
- Greenlee R. T., Hill-Harmon M. B., Murray T., et coll. Cancer statistics CA. Cancer J Clin. 2001;51:15.
- Fleming I., Cooper J. S., Henson D. E., et al. AJCC Cancer Staging anuel. Amérique conjointe Comité sur le cancer. 1999;26(2):57 ± 61.
- Binder-Foucard F., Bossard N., Delafosse P., Belot A., Woronoff A. S., Remontet L. French network of cancer registries (Francim. Cancer incidence and mortality in France over the 1980–2012 period: solid tumors. Revue d’epidemiologie et de sante publique. 2014;62(2):95-108.
- CCSsACoC, S. Statistiques canadiennes sur le cancer 2014. Toronto, ON: Société canadienne du cancer. 2014.
- Maamri A. Données épidémiologiques sur le cancer dans le monde et au Maroc. 1(1):20-29. 2015-21 Annales des Sciences de la Santé, ISSN: 2421-8936.
- Dubey M., Mohanty S. K. Age and sex patterns of premature mortality in India. BMJ Open. 2014;4(8):11.
- Sun K. Y.L et al., Les années de vie potentielle perdues avant l’âge de 65 ans Polynésie française, 2005-2010. 2014;12:1-3.
- Cruz C. S. D., Tanoue L. T., Matthay R. A. Lung Cancer: Epidemiology, Etiology, and Prevention. Clin Chest Med. 2011;32(4):605–44.
- Arfaoui A.,Soulaymani A., Habib F., et al. Epidémiologie du cancer pulmonaire au Maroc. Etude sur l’échantillon : Centre d’Oncologie Al Azhar de Rabat. Oncologie Clinique en Afrique (Maroc, 2008). 4:1.
- F. X and Cardis. “Black tobacco and cancer : introducing and epidemiological review”. European Journal of Cancer. 1991;27:1345-1348.
- Leon M. E and Dresler C. M. “Bénéfices de l’arrêt du tabac.” Bull Epidemiol Heb. 2008;21:194-198.
- Hill C., Jougla E., F Beck – point sur l’épidémie de cancer du poumon dû au tabagisme, Bulletin Epidémiologique. 2010. Special issue n° 19-20 – World No Tobacco Day, 25 May 2010.
- Mao Y., MD,Yang D.,MD, He J.,MD, Krasna J. M., MD. Epidemiology of Lung Cancer, surgical oncology clinics Surg. Oncol Clin N Am. 2016;25:439–445.
- Youlden R. D., BSc, Cramb M. S.,MPH and Baade D. P., PhD. International Epidemiology of Lung Cancer Geographical Distribution and Secular Trends. Journal of Thoracic Oncology. 2008;3(8):819–831.
- Faou L. L.,Scemama O. Épidémiologie du tabagisme Revue des Maladies respiratoires. 2005;22:8S27-8S32.
- Noureddine R., Gharnaout M & Jaafar M. Étude comparative entre le cancer bronchique chez l’homme et la femme. Revue des Maladies Respiratoires. 2015;32:A132.
- Baliunas D., Patra J., Rehm J., Popova S., Kaiserman M & Taylor B. Mortalité et années potentielles de vie perdues en raison du tabagisme au Canada en 2002: Conclusions tirées dans l’optique de la prévention et des politiques. Maladies chroniques au Canada. 2007;27(4):168.
- Lachgar A., Sahli N., Toulba A., Kebdani T., Benjaafar N. Cancer pulmonaire: parcours de soins au service de radiothérapie à l’institut national d’oncologie de Rabat. The Pan African Medical Journal. 2015;21:253. doi:10.11604/pamj.2015.21.253.6627.

This work is licensed under a Creative Commons Attribution 4.0 International License.



