

How to Cite | Publication History | PlumX Article Matrix
Shaukat Ali1 , Diwan Israr khan2*, Swaleha Akhtar2, Musab Siddiqui2
, Diwan Israr khan2*, Swaleha Akhtar2, Musab Siddiqui2
Jawahar Lal Nehru Medical College, A.M.U, Aligarh, U. P, India.
Ajmal Khan Tibbiya College and Hospital, A.M.U, Aligarh, U. P, India.
Corresponding Author E-mail: Israrjnmch@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/3116

ABSTRACT: Background: Vitamin D supplements are necessary for breastfed newborns, although little is known regarding the effectiveness of AAP’s recommended dose of 400 IU per day of it. This randomized controlled trial evaluates the efficacy of above-mentioned dose. Method: Exclusively breastfed newborns (N=28) were block randomized in two groups, vitamin D supplemented (VitD-S) and without supplement (VitD-U), 400IU/day of vitamin D is provided to Vit D-S. Serum vitamin D was assessed at the enrolment and at 3 months. Results: Vitamin D level compared between two groups, in Vit D-S at birth it was 20.4±8.7ng/ml and at 3 months it rises to 24.8±6.1ng/ml while in Vit D-U fall in level is seen from 21.4±7.8ng/ml to 14.0±5.1ng/ml which is statistically significant (p<0.001). Conclusion: Vitamin D is deficiency is quite common among mothers and babies in this location, and supplementing with 400 IU of vitamin D per day increased 25(OH)D levels in the plasma.
KEYWORDS: Breastfed; Deficiency; Newborns; Vitamin D
Download this article as:| Copy the following to cite this article: Ali S, Khan D. I, Akhtar S, Siddiqui M. To Check the Efficacy of American Academy of Paediatrics (AAP) Recommended Dose of Vitamin D in Healthy Breastfed Newborns. Biosci Biotech Res Asia 2023;20(2). |
| Copy the following to cite this URL: Ali S, Khan D. I, Akhtar S, Siddiqui M. To Check the Efficacy of American Academy of Paediatrics (AAP) Recommended Dose of Vitamin D in Healthy Breastfed Newborns. Biosci Biotech Res Asia 2023;20(2). Available from: https://bit.ly/43r1O9h |
Introduction
There are just a few foods that contain vitamin D, a fat-soluble vitamin that is also sold as a supplement. “The vitamin D we get from the sun, diet, or supplements is inactive until it passes through two hydroxylations, the first in the liver to produce 25(OH)D -Calcidiol and the second in the kidneys to produce 1,25(OH)D -Calcitriol1. Vitamin D is essential for maintaining blood calcium and phosphorus levels, bone growth, homeostasis, and musculoskeletal health. It also helps to fight against rickets and osteomalacia. Serum 25(OH)D, which has a half-life of 15 days, is the greatest indicator of vitamin D status; however, the active form of vitamin D is 1,25(OH)D.
Vitamin D status of newborns and growing fetuses depend on the maternal vitamin D level. According to studies, vitamin D deficiency in pregnant women is linked to low vitamin D levels in their children, and vitamin D dosages more than 1000 IU/day are needed to attain a 25(OH)D concentration of >50 nmol/l. Despite a surge in the percentage of children lacking enough vitamin D from 28% in 1990 to 50% in 2000,2,3. Because mothers and babies get inadequate vitamin D supplements while exclusively nursing, they are at great risk for developing major health issues. If the mother has dark skin, seldom goes outdoors, is a vegetarian, lacking dairy products, or does not get enough vitamin D herself, she runs a higher chance of both her nursing child and herself being deficient in the vitamin.4,5,6. Human milk contains 25IU/l of Vit D or less thus adequate intake cannot be met with breastfeeding7. Thus, it is necessary to supplement infants.
The American Academy of Paediatrics (AAP) advises giving all breastfed newborns 400 IU of vitamin D every day for the first six months of life. Researchers Ekhard E. Ziegler8 and colleagues from the University of Lowa compared the effectiveness of four different vitamin D dosages and discovered that the higher doses (600 and 800 IU/day) were better to the lower ones (200 and 400 IU/day). However, both of the lower doses appeared to be equally efficient and sufficient in maintaining vitamin D status, there is little evidence from Indian research to support the larger dosage as sufficient1. Thus, the objectives of our study are to assess the 25(OH)D level in healthy terms adequate for Gestational age infant at birth and to assess the impact of vitamin D on 25(OH)D.
Material methods
Study design and setting
The research involved a randomized controlled trial. The study was conducted at J.N. Medical College and Hospital at the Neonatal Unit of the Department of Paediatrics and the Department of Biochemistry between October 2011 and November 2012. J.N. Medical College and Hospital’s institutional ethics committee gave the approval for this protocol. (Appendix-1).
Sample size
The baseline prevalence of vitamin D deficiency in breastfed babies is thought to be 60%. We would need to randomly assign 14 patients to the Vit D-S and Vit D-U groups in order to decrease the prevalence of vitamin D insufficiency from 60% to 15% with 80% power and 5% significance.
Inclusion and Exclusion criteria
The term, healthy, appropriate for GA babies of <72 hrs old born at JNMCH and exclusively breastfed and likely to continue to follow up are included. Subjects whose mothers have any chronic illness, are unwilling or unable to continue breastfeeding, have any congenital abnormality in infants, or have an illness requiring hospitalisation in the neonatal period, particularly CKD and RTA, are excluded. Other exclusion criteria include living more than 100 kilometres away from the study site and being unlikely to be followed up.
Trial deviates
For those who fail to exclusively breastfeed their babies, regular use (constituting more than 2 feeds a day) of supplemental milk from other sources for more than 3 days. Missing doses of vitamin D for more than 7 days.
Procedure
During the study period a total of 50 mother-infant pairs were assessed for eligibility for the study, out of which 32 mother-infant pairs met the eligibility criteria and were considered for recruitment in the study (figure-1). Four infants were excluded because of their inability to continue breastfeeding or unlikely to follow up at the hospital. Informed consent was taken from the remaining 28 infants for participating in the study (Appendix-2). These 28 infants were randomized to either Vitamin D- supplemented group (VitD-S, n=14) or the vitamin D unsupplemented group (VitD-U; n=14) groups. Demographic and antenatal data were recorded and a detailed examination including anthropometry was done. In addition to measuring the mothers’ height, weight, and BMI, researchers also recorded the mothers’ calcium and vitamin supplemental intake during and after delivery. Block randomization was done for allocation of subjects to either Vit D-S or Vit D-U group. In the Vit D-S group, Vitamin D drop was provided and the mother was instructed to administer vitamin D in a dose of 1ml (400IU) daily for 3 months.
Blood collection
Both the mother and the infant had 4ml of blood collected at the time of enrolment to measure their serum levels of 25(OH)D, calcium, phosphorus, and alkaline phosphatase. 4 ml of blood were once more taken from neonates for the same investigation to assess the outcome.
Laboratory methods
We used a colorimetric assay to measure serum alkaline phosphatase, a blood gas electrolyte analyzer to measure serum calcium, a UV end point assay kit to evaluate serum phosphorus, and an ELISA assay kit to measure serum 25(OH)D9.
Follow -up
At age of 6wks, 10wks, and 14wks. In the Vit D-S group counselling for exclusive breastfeeding was done and immunisation was also checked. In Vit D-U group check for any use of vitamin D supplements from other sources.
Statistical analysis
One-way analysis of variance (ANOVA) tests and independent t-tests were used to assess the differences between groups in blood 25(OH)D, calcium, phosphorus, alkaline phosphatase, and other secondary variables. Serum 25(OH)D concentrations under 15 ng/ml were used to indicate vitamin D deficiency.
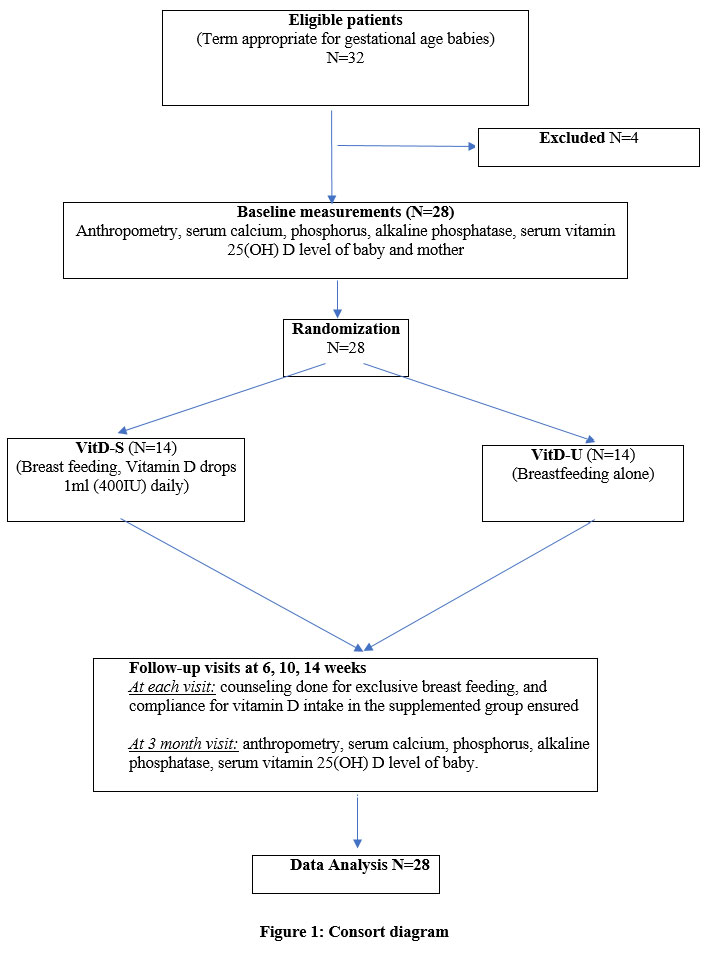 |
Figure 1: Consort diagram |
Observations and result
A total of 50 mother-infant pairs were evaluated for research eligibility, and 32 of those mother-infant couples passed the test and were given a green light to be included in the study. Of these 4 infants were excluded, and the remaining 28 infants participated in the study. These 28 students were randomized into Vit D-S and Vit D-U group, and Vit D-S group were administered with 400IU/day of vitamin D, both groups were exclusively breastfed.
When clinical data, such as age, sex, birth weight, length, head circumference, and chest circumference, were assessed at enrolment, there were no statistically significant differences between the groups. At enrolment, the mother’s clinical features were also evaluated, although no significant changes were found. The difference in blood vitamin D levels between the two groups at birth was statistically significant (p0.001): the Vit D-S group had 20.4 ng/ml at birth which rises to 24.8 ng/ml after 3 months, while the Vit D-U group had 21.4 ng/ml at birth and 14.0 ng/ml at 3 months in the Vit D-S group (Fig 2 & Table 1).
Serum vitamin D levels in the Vit D-S group were 20.9±6.0 ng/ml, while those in the Vit D-U group were 20.7 7.1 ng/ml (P = 0.955). Vitamin D supplemented moms had lower serum calcium levels than non-supplemented mothers (9.1 vs. 9.8 mg/dl respectively, P = 0.069). In the Vit D-U group, the serum phosphorus level was 4.3±0.8 mg/dl, compared to 4.7±0.8 mg/dl in the moms of Vit D-S (P = 0.182). Serum alkaline phosphatase levels were 135.4 78.6 IU/l in mothers of vitamin D-S and 120.2 100.7 IU/l in mothers of vitamin D-U, respectively (P = 0.660). At three months and at delivery, the proportion of mothers and babies who were vitamin D deficient was compared (Table 2). Only 4 (21%) newborns were vitamin D deficient at delivery out of 19 (67.9%) moms with blood vitamin D levels of 15 ng/ml or higher. Conversely, 8 (89.9%) of the remaining 9 (32.1%) vitamin D-deficient women produced offspring who were likewise deficient at birth; odds ratio = 30 (95% CI: 2.8-315); P=0.003. Vitamin D levels were assessed in both the supplemented and control groups at birth and again at three months of age. At delivery, two of the seven babies in the Vit D-S group had low levels of vitamin D, and their levels did not rise after supplementation. Supplemented infants had a higher proportion of babies with baseline vitamin D levels of 15ng/ml or higher, and none of these babies were deficient at three months (95% CI: 0.27-172.2), odds ratio= 6.82, P=0.244. Five infants in the vitamin D-U group had deficiencies at birth that persisted at three months. Of the 9 additional infants whose serum vitamin D levels were greater than or equivalent to 15 ng/ml at birth, 5 of them exhibited deficiency symptoms by three months (Table 3, 4).
Table 1: Comparison of serum vitamin D levels at birth and 3 months in Vit D-S and Vit D-U group
|
Time |
Serum Vitamin D level (ng/ml) * |
P value |
|
|
VitD-S (N=14) |
VitD-U (N=14) |
|
|
|
· At birth |
20.4 + 8.7# [11.0 – 34.0] |
21.4 + 7.8@ [10.0 – 32.0] |
0.751 |
|
· At 3 months |
24.8 + 6.1# [13.0 – 34.0] |
14.0 + 5.1@ [8.0 – 24.0] |
<0.001 |
|
|
Figure 2: Box-Plot of serum vitamin D level at birth and 3 months |
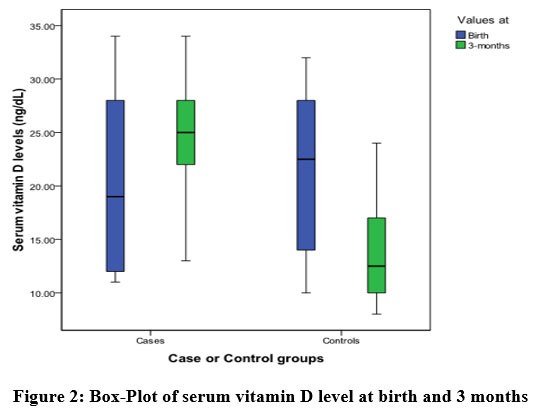
Table 2: Vitamin D deficient mothers and babies at birth and 3 month
|
|
VitD-S (N=14) |
VitD-U (N=14) |
P value |
|
Vitamin D deficient mothers |
4 (28.6) |
5 (35.7) |
0.691 |
|
Vitamin D deficient babies |
|
|
|
|
· At birth |
7 (50.0) |
5 (35.7) |
0.453 |
|
· At 3 months |
2 (14.3) |
10 (71.4) |
0.003 |
Values are n (%) of mothers or babies with serum vitamin D levels <15ng/ml
Table 3: Comparison of the vitamin D supplemented group status at birth and at three months (Vit D-S)
|
Vitamin D status at birth |
Vitamin D status at 3 months |
|
|
|
<15ng /ml |
≥ 15 ng /ml |
|
< 15 ng /ml (N=7) |
2 |
5 |
|
≥ 15 ng /ml (N=7) |
0 |
7 |
Odds ratio=6.82 (95% CI: 0.27-172.2 with), P =0.244
Table 4: Comparison of the vitamin D-unsupplemented group’s vitamin D levels at birth and at three months (Vit D-U
|
Vitamin D status at birth |
Vitamin D status at 3 months |
|
|
<15ng /ml |
≥ 15 ng /ml |
|
|
< 15 ng /ml (N=5) |
5 |
0 |
|
≥ 15 ng /ml (N=9) |
5 |
4 |
P=0.172, Odd ratio-9.0 (95% CI: 0.385-210).
Discussion
Vitamin D is synthesized endogenously and acts as a hormone in the body. In the endocrine system, vitamin D plays a number of vital biological functions, including calcium homeostasis, bone mineral metabolism, cell differentiation, suppression of cell proliferation, and immunomodulation.10,11. Our results showed an average vitamin D level of 20.9± 8.1 ng/ml (interquartile range: 10-34 ng/ml) in newborns’ blood. The vitamin D blood level in the vitamin D-supplemented group (VitD-S) was 20.4±8.7 ng/ml [range=11-34 ng/ml], while it was 21.4±7.8 ng/ml [range=10-32 ng/ml] in the vitamin D-unsupplemented group (VitD-U). In our study, moms’ vitamin D levels were 20.8±6.5 ng/ml (range 11-30 ng/ml). Bhalala et al. from India observed vitamin D levels in cord blood serum of 19.36±9.57ng/ml, which are comparable to those in our study12. In our study, vitamin D deficiency was defined as a blood vitamin D level of 15 ng/ml or less, which is the same criterion utilized in earlier Indian studies13,14. Additionally, we discovered that 32.1% of moms lack enrollment (within 3 days of delivery). 89.9% of babies born to mothers with low vitamin D levels (serum vitamin D level 15 mg/ml) had vitamin D deficiencies”. There is a significant correlation between the levels of 25(OH) D in mothers and their offspring (r =0.578, 95% CI =0.261-0.782, P 0.001). (Fig 4). From their research, Seth et al.15 (2014) in New Delhi revealed that 47.8% of mothers and 43.2% of neonates had blood 25(OH)D levels < 25 nmol/l (10 ng/ml), indicating a strong positive connection between them (r = 0.324, P 0.001). There is no evidence from any Indian research to support giving a healthy breastfed child 400 IU of oral vitamin D3. The VitD-S group in our research received a daily 400 IU oral vitamin D-3 supplement for three months, whereas the VitD-U group received no such supplement. In VitD-S, the prevalence of vitamin D insufficiency decreased from 50% to 14%; however, in VitD-U, it increased from 35.7 to 71.4 percentage. VitD-S patients also saw a substantial rise in their mean serum vitamin D level, from 20.4 ±8.7 ng/ml to 24.8± 6.1 ng/ml (P=0.016). The average blood vitamin D significantly improve from 16.0± 9.3 ng/ml to 43.6± 14.1 ng/ml (P≤ 0.0001) after 4 months of supplementation, according to a randomized controlled investigation by Wagner et al.16 in the United States. We discovered that 14% of infants in the VitD-S group were still deficient at three months, despite receiving daily 400 IU oral vitamin D3 supplementation. Given the high rate of vitamin D deficiency among Indian moms, 400 IU of oral vitamin D-3 per day may not be sufficient to prevent vitamin D deficiency in all breastfed Indian neonates, at least in this area. In the VitD-U group, vitamin D insufficiency increased from 35.7% to 71.4% over the course of three months. In addition, the control group’s mean blood vitamin D level decreased significantly (P <0.001) from 21.4 ± 7.8 to 14.0 ± 5.1 ng/ml. There has been a lot of discussion about vitamin D deficiency in otherwise healthy term-breastfed 3-month-old neonates and their mothers [serum 25 hydroxyvitamin D (25OHD) 15 ng/ml]. Jain and colleagues from New Delhi17 claim the following, they discovered extraordinarily high figures of 66.7% vitamin D deficiency in babies and 81.1% of women studied, which is consistent with other studies from other parts of India.
There are certain limitations to this study. Firstly, we are unable to extend the study period to 6-months as it would be interesting to see if the deficiency noted despite vitamin D supplementation abates after continued supplementation beyond 3 months. Financial constraints also did not permit us from measuring concomitant serum parathormone levels, we were unable to check for radiological evidence of rickets in the deficient population.
Conclusion
According to the study’s results, vitamin D insufficiency is a common problem among local expecting mothers and their unborn children. It is feasible to raise blood vitamin D levels after three months with 400 IU of vitamin D per day, but it may not be enough to fully correct the vitamin D insufficiency that was detected at that time. Vitamin D status of mother also affect the vitamin D status of newborns18,19. However, we are not estimated Vitamin D status of mother in this study More research is needed to determine if 400 IU of vitamin D per day is enough or whether vitamin D supplementation for expectant and nursing mothers, as well as optimal sun exposure for new-born’s, are necessary to prevent any kind of vitamin D deficiency in breastfed babies.
Acknowledgement
I cannot express enough thanks to my committee for their continued support and encouragement.
Conflict of Interest
The authors have no conflict of interest.
Funding sources
We have not received any funding for the study.
References
- Wagner CL, Greer FR. American academy of pediatrics on Breastfeeding and Committee on Nutrition. Prevention of Rickets and Vitamin D Deficiency in Infants, Children, and Adolescents. Pediatrics 2008;122:1142-1152.
CrossRef - Moncrieff M, Fadahunsi TO. Congenital rickets due to maternal vitamin D deficiency. Arch Dis Child 1974;49:810-1.
CrossRef - Markestad T, Aksnes L, Ulstein M, Aarskog D. 25-Hydroxyvitamin D and 1,25-dihydroxy,vitamin D of D2 and D3 origin in maternal and umbilical cord serum after vitamin D2 supplementation in human pregnancy. Am J Clin Nutr. 1984 Nov;40(5):1057-63.
CrossRef - Kreiter SR, Schwartz RP, Kirkman HN Jr, Charlton PA, Calikoglu AS, Davenport Nutritional rickets in African American breast-fed infants. J Pediatr. 2000;137:153–157.
CrossRef - Salle BL, Glorieux FH, Lapillone A. Vitamin D status in breastfed term babies. Acta Pediatr 1998;87: 726-727.
CrossRef - Greer FR. Vitamin D deficiency–It’s more than rickets. J Pediatr 2003; 143:422-423.
CrossRef - Daaboul J, Sanderson S, Kristensen K, Kitson H. Vitamin D deficiency in pregnant and breastfeeding women and their infants. J Perinatol 1997;17:10-4.
- Ekhard E. Ziegler1, Steven E. Nelson1 and Janice M. Jeter Vitamin D supplementation of breastfed infants: a randomized dose–response trial; Volume 76; Number 2; August 2014 Pediatric Research.
CrossRef - Nicolas Heureux, Ernst Lindhout , Leon Swinkels -A direct assay for measuring Free 25 Hydroxyvitamin D ; J AOAC Int. 2017 Sep 1;100(5):1318-1322.
CrossRef - Holick MF. Vitamin D: the underappreciated D-lightful hormone that is important for skeletal and cellular health. Curr Opin Endocrinol Diabetes 2000;9:87–98.
CrossRef - Veldman CM, Cantorna MT, DeLuca HF. Expression of 1,25- dihydroxvatamin D3 receptor in the immune system. Arch Biochem Biophys 2000;374:334-8.
CrossRef - Bhalala U, Desai M, Parekh P, Mokal R, Chheda B. Subclinical Hypovitaminosis D Among Exclusively Breastfed Young Infants, Indian pediatrics, 2007; volume 44 December17:897-901
- Balasubramanian K, Rajeswari J, Gulab, et al.Varying role of vitamin D deficiency in the etiology of rickets in young children vs. adolescents in northern India. J Trop Pediatr. 2003;49(4):201-6.
CrossRef - Shaikh U, Alpert PT. Nutritional rickets in Las Vegas, Nevada. J Pediatr Endocrinol Metab. 2006; 19(3):209–212.
CrossRef - Seth A, Marwaha RK, Singla B, et al.Vitamin D nutritional status of exclusively breastfed infants and their mothers. J Pediatr Endocrinol Metab.2009Mar;22(3):241-6.
CrossRef - Wagner CL, Howard C, Hulsey TC, et al. Circulating 25-Hydroxyvitamin D Levels in Fully Breastfed Infants on Oral Vitamin D Supplementation. International Journal of Endocrinology,2010;4:1-5.
CrossRef - Jain V, Gupta N, Kalaivani M, Jain A, Sinha A, Agarwal R. Vitamin D deficiency in healthy breastfed term infants at 3 months & their mothers in India: seasonal variation and determinants. Indian J Med Res 2011; 133:267-73.
- Prasanna Naik, M M A Faridi , Prerna Batra , S V Madhu-Oral Supplementation of Parturient Mothers with Vitamin D and Its Effect on 25OHD Status of Exclusively Breastfed Infants at 6 Months of Age
- Adekunle Dawodu , Khalil M Salameh , Najah S Al-Janahi , Abdulbari Bener , Naser Elkum– The Effect of High-Dose Postpartum Maternal Vitamin D Supplementation Alone Compared with Maternal Plus Infant Vitamin D Supplementation in Breastfeeding Infants in a High-Risk Population

This work is licensed under a Creative Commons Attribution 4.0 International License.



