

How to Cite | Publication History | PlumX Article Matrix
State of Adenosine Deaminase in Patients with Dyslipidemia
Amit Kumar Yadav1 , Saba Khan1 , Shubhra Chowdhry2, Rohit Kumar Srivastava3, Roshan Alam1and Mohammad Mustufa Khan4*
, Saba Khan1 , Shubhra Chowdhry2, Rohit Kumar Srivastava3, Roshan Alam1and Mohammad Mustufa Khan4*
1Department of Biochemistry, Integral Institute of Medical Sciences and Research (IIMSR), Integral University, Lucknow, Uttar Pradesh, India.
2Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India.
3Department of Paramedical Sciences, Mahayogi Gorakhnath University, Gorakhpur, Uttar Pradesh, India.
4Department of Basic Medical Sciences, Integral Institute of Allied Health Sciences & Research (IIAHSR), Integral University, Lucknow, Uttar Pradesh, India
Corresponding Author E-mail: mustufakhan@iul.ac.in
DOI : http://dx.doi.org/10.13005/bbra/3292

ABSTRACT: Background: Dyslipidemia is becoming more common across all age groups mainly in young individuals because of imbalanced diets, low physical activity, and sedentary work culture. Several studies reported that elevated serum adenosine deaminase activity was associated with dyslipidemia, but the results were not consistent. Aim: It is aimed to correlate adenosine deaminase and lipid profile parameters in patients with dyslipidemia. Material and Methods: In this case-control study, a total of 60 subjects (30 diagnosed dyslipidemia patients and 30 age and gender-matched healthy individuals) were enrolled. Serum lipid profile parameters and adenosine deaminase levels were estimated in each subject. Results: The mean levels of lipid profiles, mainly triacylglycerol (TG), low-density lipoprotein-cholesterol (LDL-C), and adenosine deaminase, were found to be significantly high, while high-density lipoprotein-cholesterol (HDL-C) was found significantly low in cases than controls (p <0.001). adenosine deaminase has not shown any significant correlation with lipid profile parameters in patients with dyslipidemia and controls. Conclusion: The result showed that the serum adenosine deaminase and serum lipid profile levels were altered in patients with dyslipidemia.
KEYWORDS: Adenosine; Adenosine Deaminase; Case-Control Study; Dyslipidemia; Lipid Profile
Download this article as:| Copy the following to cite this article: Yadav A. K, Khan S, Chowdhry S, Srivastava R. K, Alam R, Khan M. M. State of Adenosine Deaminase in Patients with Dyslipidemia. Biotech Res Asia 2024;21(3). |
| Copy the following to cite this URL: Yadav A. K, Khan S, Chowdhry S, Srivastava R. K, Alam R, Khan M. M. State of Adenosine Deaminase in Patients with Dyslipidemia. Biotech Res Asia 2024;21(3). Available from: https://bit.ly/3U4Bkbo |
Introduction
Dyslipidemia is becoming more common across all age groups mainly in young individuals, because of imbalanced diets, low physical activity, and sedentary work culture1,3. Dyslipidemia was linked to an increased risk of developing atherosclerotic coronary and peripheral arterial disease as well as cardiovascular diseases (CVD) in later life2. About 30% of the urban and 20% of the rural population of India is living with dyslipidemia4. Joshi et al reported that the prevalence of hypercholesterolemia and hypertriglyceridemia was found 13.9% and 29.5%, respectively. In addition, low high-density lipoprotein-cholesterol (HDL-C) was 72.3%, high low-density lipoprotein-cholesterol (LDL-C) was found at 1.8%, and 79% had shown lipid abnormalities in any one parameter of lipid profile in the Indian population5. The National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP-III) criteria were used to classify dyslipidemia; when total cholesterol (TC)>200 mg/dl or LDL-C >130 mg/dl indicated hypercholesterolemia, while HDL-C <40 mg/dl indicated hypercholesterolemia. A diagnosis of hypertriglyceridemia was made when the plasma triglyceride (TG) level was more than 150 mg/dl6. Elevated TC and reduced HDL-C levels have been found in Asian Indians as compared to other ethnic groups7,8.
Adenosine deaminase (ADA) is an enzyme of the purine catabolism pathway that converts adenosine to inosine by deamination9. It is expressed in various cells and tissues and plays a significant role in the proliferation and maturation of lymphocytes, monocytes, and macrophages10. Adenosine suppresses glycogen synthesis and stimulates glycogenolysis in hepatic cells11. Adenosine regulates cholesterol synthesis by the liver and affects circulatory levels of TC and TG and fat tissue amounts12. ADA activity has been associated with obesity13, obesity-associated complications14, type 2 diabetes mellitus (T2DM)15, and CVD16,17, illustrated in Figure 1.
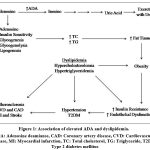 |
Figure 1: Association of elevated ADA and dyslipidemia. |
Asian Indians are more prone to dyslipidemia and its-associated complications that increase the risk factors for coronary artery disease (CAD) and CVD. Studies reported that elevated serum adenosine deaminase (ADA) activity was associated with dyslipidemia, but results were not consistent. We aimed to correlate ADA and lipid profile parameters in patients with dyslipidemia.
Materials and Methods
Selection of Subject
Thecase-control study included 60 subjects (30 diagnosed dyslipidemia patients and 30 age and gender-matched controls) were included aged 25-60 years from the University Medical Hospital OutPatient Department (OPD) of Medicine. A detailed demographical and medical history has been taken from each subject. Informed written consent was taken from each study subject.
Inclusion of Subject
Cases were diagnosed as per the guidelines of NCEP ATP-III6.
Exclusion of Subject
The subject has a medical history of type 1 or type 2 diabetes mellitus (type 1 or type 2), CVD, CAD, chronic kidney disease (CKD), liver cirrhosis, thyroid disorders, and infectious diseases such as tuberculosis, HIV, sexually transmitted diseases, hepatitis, and pregnant or lactating women were excluded from the study. The subject who was taking lipid-lowering medicine, such statin, was also excluded.
Collection of Sample
A total of 4 ml of peripheral venous blood was collected from each study subject in a plain vial after an overnight after 12 hours of fasting. It was centrifuged at 3000-4000 rpm for 5-10 min and the serum was separated and stored in a deep freezer (-20 °C) till further laboratory investigation.
Laboratory Investigation
ADA, TC, TG, and HDL-C were measured using the colorimetric method utilizing commercially available kits in Chemistry Semi-auto analyzer (Chem-7, Erba Diagnostics Pvt Ltd, Germany). LDL-C and VLDL-C were calculated by using Friedewald’s formula18-21.
Statistical Analysis
SPSS software (version 20.0) was used. Data were represented as Mean ± Standard deviation (SD). All quantitative clinical parameters were calculated in dyslipidemia patients and healthy control subjects. A p-value was calculated using a student unpaired t-test. A correlation analysis was performed on ADA and lipid profile parameters among cases and controls. A p-value (<0.05) was considered statistically significant.
Results
Results showed that the mean levels of lipid profiles mainly TG and LDL-C and the ADA were found significantly elevated and HDL-C levels reduced in cases than controls (p<0.001), shown in Table 1. Mean of ADA levels in cases and controls is shown in Figure 2.
Table 1: Clinical characteristics of cases and controls
| Parameters | Cases(Mean ± SD)(n= 30) | Controls(Mean ± SD)(n= 30) | p-value |
| Age (years) | 34.10±9.84 | 34.5±9.69 | 0.87 |
| Gender (M/F) | 22/8 | 20/10 | 0.78 |
| TC (mg/dL) | 256.12± 20.73 | 152.60 ± 26.42 | <0.001* |
| TG (mg/dL) | 159.63 ±40.91 | 100.93 ± 26.43 | <0.001* |
| HDL-C (mg/dL) | 40.20±6.27 | 51.23 ± 10.08 | <0.001* |
| LDL-C (mg/dL) | 103.03± 15.09 | 81.51± 21.22 | <0.001* |
| VLDL-C (mg/dL) | 32.04± 8.15 | 20.24± 5.28 | <0.001* |
| ADA (IU/L) | 35.22± 3.03 | 17.93 ± 5.32 | <0.001* |
| Data represented as Mean ±SD.*p-value (< 0.05), considered statistically significant. ADA: Adenosine Deaminase, HDL-C: High-Density Lipoprotein-Cholesterol, LDL-C: Low-Density Lipoprotein-Cholesterol, VLDL-C: Very Low-Density Lipoprotein-Cholesterol, TG: Total Triglyceride, TC: Total Cholesterol | |||
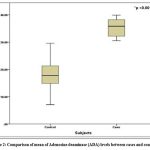 |
Figure 2: Comparison of mean of Adenosine deaminase (ADA) levels between cases and controls. |
Results showed that ADA has not shown any significant association with lipid profile parameters in patients with dyslipidemia and controls as shown in Table 2.
Table 2: Correlation of ADA (IU/L) and lipid profile among cases and controls
| Parameters | Case(r) | Control(r) |
| Age (years) | -0.014 | 0.034 |
| TC(mg/ dL) | -0.249 | -0.051 |
| TG(mg/dL) | 0.217 | -0.160 |
| HDL-C(mg/dL) | -0.226 | 0.037 |
| LDL-C(mg/dL) | -0.302 | -0.042 |
| VLDL-C(mg/dL) | 0.221 | -0.159 |
| ** 0.01 or *0.05 level (2-tailed) was considered significant correlation.ADA: Adenosine Deaminase. HDL-C: High-Density Lipoprotein-Cholesterol, LDL-C: Low Density Low-Density Lipoprotein-Cholesterol, TG: Total Triglyceride, TC: Total Cholesterol, VLDL-C: VLDL-C: Very Low Density Lipoprotein-Cholesterol | ||
Discussion
Results showed that the mean levels of lipid profiles and ADA were found significantly elevated, while HDL-C was significantly reduced in cases than controls (p<0.001). Elevated lipid profiles mainly LDL-C and TG and decreased HDL-C in the blood are the primary diagnostic criteria of dyslipidemia22. Studies reported that mean levels of ADA were found to be significantly high in patients with dyslipidemia23,24.
Results showed that ADA has not shown any significant association with lipid profiles in patients with dyslipidemia and controls. Similarly, ADA has not shown any significant association with lipid profiles in patients with dyslipidemia23. However, it was reported that ADA has a significant association with hypercholesterolemia and LDL-C25. In addition, it was reported that serum ADA has shown a significant relationship with coronary artery calcification in patients with T2DM26. It was further suggested that ADA should be considered as a biomarker for atherosclerosis severity in patients with T2DM.
Abnormal TG and HDL-C levels are the main parameters for the diagnosis of metabolic syndrome along with fasting blood sugar, blood pressure, and waist circumference6,27. Dyslipidemia is a predictor of CVD and CAD. It is a leading cause of atherosclerosis and the pathophysiology of CVD2. Age shifting pattern was observed in the incidence of CVD and its associated mortality in the Indian population. The incidence of heart attack (10%) was observed in young individuals (< 40 years) and more than 50% of CVD-associated deaths were observed in old individuals (>70 years). CVD and CAD-associated deaths were three-fold higher in the Indian population than in other developed countries28,29.
It is necessary to find new markers that can be used for early screening of dyslipidemia and its associated pathophysiology such as atherosclerosis, CVD, and CAD in the Indian population. ADA may play a significant role in this regard. However, ADA is a predictor of hyperglycemia and regulates insulin sensitivity. ADA activity increases with increasing glycated hemoglobin (HbA1c) in patients with T2DM15. Hyperglycemia causes an abnormal lipid profile, which resulting hypercholesterolemia and dyslipidemia30. In addition, oxidative stress triggers lipid peroxidation in patients with dyslipidemia which is a form of the oxidative marker malondialdehyde (MDA). Elevated MDA levels were reported in patients with hypertension and T2DM31,32. Hypertension and T2DM increase 2-4 times the risk of CVD, atherogenic dyslipidemia, and their associated morbidity and mortality33.
Conclusion
The result showed that the serum ADA and serum lipid profile levels were altered in patients with dyslipidemia. This suggested that serum ADA levels to be assessed in dyslipidemia patients to redcue the further complications.
Limitations and Future Prospects of the Study
The present study used a small sample size. Further study with a large sample size is required to verify the association between ADA and dyslipidemia. Because elevated ADA activity reduces the levels of adenosine by deamination. However, Adenosine regulates glucose and lipid metabolism. Elevated ADA activity and diminished adenosine levels altered the glucose and lipid metabolism resulting in dyslipidemia, T2DM, and CVD12.
Acknowledgement
We are grateful to the Prof. (Dr.) Abha Chandra, Dean, Integral Institute of Medical Sciences & Research (IIMSR) for the invaluable help and encouragement to carry out research work without any hindrance.
Conflicts of Interest
Authors declared that they have no conflict of interest
Funding Sources
This study was not funded by any funding agency or company.
Data Availability Statement
This statement does not apply to this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (IEC Approval No. IEC/IIMS&R/2022/16) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Written informed consent was obtained from all individual participants included in the study.
Reference
- Park JH, Moon JH, Kim HJ, Kong MH, Oh YH. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J Fam Med. 2020 Nov;41(6):365-373. doi: 10.4082/kjfm.20.0165.
CrossRef - Misra S, Lyngdoh T, Mulchandani R. Guidelines for dyslipidemia management in India: A review of the current scenario and gaps in research. Indian Heart Journal. 2022 Aug 5. https://doi.org/10.1016/j.ihj.2022.07.009.
CrossRef - LAI: Lipid Association of India Expert Consensus Statement on Management of Dyslipidemia in Indians 2020: Part III. Supplement to Journal of the Association of Physicians of India. Published on 1st of Every Month 1st November, 2020 [Available at http://www.lipid.net.in/wp-content/uploads/2021/02/FinalJAPIfullconsensusstatement.pdf]
- NHP: National Health Portal admin. Dyslipidemia. Published and last updated on 05 April 2019. Last accessed on 06 October 2022 [Available at https://www.nhp.gov.in/dyslipidemia_ mtl#:~:text=In%20India%20approximately%2025%2D30,subjects%20are%20suffering%20from%20dyslipidaemia.].
- Joshi SR, Anjana RM, Deepa M, Pradeepa R, Bhansali A, Dhandania VK, Joshi PP, Unnikrishnan R, Nirmal E, Subashini R, Madhu SV, Rao PV, Das AK, Kaur T, Shukla DK, Mohan V; ICMR-INDIAB Collaborative Study Group. Prevalence of dyslipidemia in urban and rural India: the ICMR-INDIAB study. PLoS One. 2014 May 9;9(5):e96808.
CrossRef - NCEP: National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002 Dec 17;106(25):3143-421.
CrossRef - Gupta R, Rao RS, Misra A, Sharma SK. Recent trends in epidemiology of dyslipidemias in India. Indian Heart J. 2017 May-Jun;69(3):382-392. doi: 10.1016/j.ihj.2017.02.020.
CrossRef - Nirwan R, Singh D. Distribution of lipids and prevalence of dyslipidemia among Indian expatriates in Qatar. Journal of lipids. 2021 Mar 5;2021:1-9. https://doi.org/10.1155/2021/8866784.
CrossRef - Cortés A, Gracia E, Moreno E, Mallol J, Lluís C, Canela EI, Casadó V. Moonlighting adenosine deaminase: a target protein for drug development. Medicinal research reviews. 2015 Jan;35(1):85-125.
CrossRef - Flinn AM, Gennery AR. Adenosine deaminase deficiency: a review. Orphanet journal of rare diseases. 2018 Dec;13(1):1-7.
CrossRef - Yasuda N, Inoue T, Horizoe T, Nagata K, Minami H, Kawata T, Hoshino Y, Harada H, Yoshikawa S, Asano O, Nagaoka J. Functional characterization of the adenosine receptor contributing to glycogenolysis and gluconeogenesis in rat hepatocytes. European journal of pharmacology. 2003 Jan 17;459(2-3):159-66.
CrossRef - Koupenova M, Ravid K. Adenosine, adenosine receptors and their role in glucose homeostasis and lipid metabolism. J Cell Physiol. 2013 Mar 4:10.1002/jcp.24352. doi: 10.1002/jcp.24352.
CrossRef - Jadhav AA, Jain A. Elevated adenosine deaminase activity in overweightand obese Indian subjects. Archives of physiology and Biochemistry. 2012 Feb 1;118(1):1-5.
CrossRef - Bernhardt GV, Shivappa P, Bernhardt K, Bhat S, Pinto JR, Jhancy M, Kumar S. Markers of inflammation in obese pregnant women: Adenosine deaminase and high sensitive C–reactive protein. European Journal of Obstetrics & Gynecology and Reproductive Biology: X. 2022 Dec 1;16:100167.https://doi.org/10.1016/j.eurox.2022.100167.
CrossRef - Niraula A, Thapa S, Kunwar S, Lamsal M, Baral N, Maskey R. Adenosine deaminase activity in type 2 diabetes mellitus: does it have any role?. BMC endocrine disorders. 2018 Dec;18:1-5. https://doi.org/10.1186/s12902-018-0284-9.
CrossRef - Xuan C, Tian QW, Zhang SY, Li H, Tian TT, Zhao P, Yue K, Ling YY, He GW, Lun LM. Serum adenosine deaminase activity and coronary artery disease: a retrospective case-control study based on 9929 participants. Therapeutic advances in chronic disease. 2019 Dec;10:2040622319891539. https://doi.org/10.1177/2040622319891539.
CrossRef - Kutryb-Zajac B, Mierzejewska P, Slominska EM, Smolenski RT. Therapeutic perspectives of adenosine deaminase inhibition in cardiovascular diseases. Molecules. 2020 Oct 12;25(20):4652. https://doi.org/10.3390/molecules25204652.
CrossRef - Giusti G. Adenosine deaminase. In Methods of enzymatic analysis 2nd Edition, Volume 2, 1974 Jan 1 (pp. 1092-1099). Academic Press. ISBN: 978-0-12-091302-2. https://doi.org/10.1016/B978-0-12-091302-2.50108-0.
CrossRef - Cooper GR, Myers GL, Smith SJ, Schlant RC. Blood lipid measurements: variations and practical utility. Jama. 1992 Mar 25;267(12):1652-60. DOI:10.1001/jama.1992.03480120090039.
CrossRef - Mora S, Rifai N, Buring JE, Ridker PM. Comparison of LDL cholesterol concentrations by Friedewald calculation and direct measurement in relation to cardiovascular events in 27 331 women. Clinical chemistry. 2009 May 1;55(5):888-94.
CrossRef - Dubba MR, Ramyashree V, Harshitha SS, Biswas M, Shenoy RP, Suryakanth VB. Efficiency of Galanti and Guisti Method of ADA Estimation in Comparison with the Gold Standard. Ethiop J Health Sci. 2020 Nov;30(6):897-902. doi: 10.4314/ejhs.v30i6.7.
CrossRef - Mosca S, Araújo G, Costa V, Correia J, Bandeira A, Martins E, Mansilha H, Tavares M, Coelho MP. Dyslipidemia Diagnosis and Treatment: Risk Stratification in Children and Adolescents. J NutrMetab. 2022 Feb 21;2022:4782344. doi: 10.1155/2022/4782344.
CrossRef - Khan MR, Babu SV, KuzhandaiVelu V. Association of serum adenosine deaminase level with atherosclerotic index in type 2 diabetes mellitus patients. Biomedicine. 2021 Apr 3;41(1):150-2.
CrossRef - Anand AK, Mustafa A. Role of adenosine deaminase in dyslipidemia. International Journal of Health Sciences. 2022;6:5752-8. https://doi.org/10.53730/ijhs.v6nS4.10167.
CrossRef - Nwankwo AA, Osim EE, Bisong SA. Contributory role of adenosine deaminase in metabolic syndrome. Nigerian Journal of Physiological Sciences. 2013;28(1):73-6.
- Yu M, Zhou H, Li Q, Ding J, Shuai H, Zhang J. Serum adenosine deaminase as a useful marker to estimate coronary artery calcification in type 2 diabetes mellitus patients. Clinical and Applied Thrombosis/Hemostasis. 2021 Feb 28;27:1076029621999722.
CrossRef - Zhang L, Wang H, Ma Q, Liu Y, Chen A, Lu J, Ren L. Value of the triglyceride–glucose index and non-traditional blood lipid parameters in predicting metabolic syndrome in women with polycystic ovary syndrome. Hormones. 2023 Feb 15:1-9.https://doi.org/10.1007/s42000-023-00438-6.
CrossRef - Chandra KS, Bansal M, Nair T, Iyengar SS, Gupta R, Manchanda SC, Mohanan PP, Rao VD, Manjunath CN, Sawhney JP, Sinha N, Pancholia AK, Mishra S, Kasliwal RR, Kumar S, Krishnan U, Kalra S, Misra A, Shrivastava U, Gulati S. Consensus statement on management of dyslipidemia in Indian subjects. Indian Heart J. 2014 Dec;66Suppl 3(Suppl 3):S1-51. doi: 10.1016/j.ihj.2014.12.001.
CrossRef - Prabhakaran D, Jeemon P, Sharma M, Roth GA, Johnson C, Harikrishnan S, Gupta R, Pandian JD, Naik N, Roy A, Dhaliwal RS. The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990–2016. The Lancet Global Health. 2018 Dec 1;6(12):e1339-51. https://doi.org/10.1016/S2214-109X(18)30407-8.
CrossRef - Mooradian AD. Dyslipidemia in type 2 diabetes mellitus. Nature Reviews Endocrinology. 2009 Mar;5(3):150-9. https://doi.org/10.1038/ncpendmet1066.
CrossRef - Mishra P, Tiwari D, Khan MM, Manger PT. Evaluation of oxidative stress and dyslipidemia in diagnosed hypertensive patients. Biochem. Cell. Arch. 2019;19(2):3867-72.DOI : 10.35124/bca.2019.19.2.3867.
- Kumar S, Kumar A, Khan MM. Estimation of aldose reductase activity and malondialdehyde levels in patients with type 2 diabetes mellitus. Biomedical and Pharmacology Journal. 2019 Jun 25;12(2):1001-7.DOI: https://dx.doi.org/10.13005/bpj/1728.
CrossRef - Roman G, PanteaStoian A. Cardiovascular risk/disease in type 2 diabetes mellitus. Type 2 Diabetes: From Pathophysiology to Cyber Systems. 2021 Apr 20:277. DOI: 10.5772/intechopen.97422.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



