

How to Cite | Publication History | PlumX Article Matrix
Shafa Salahuddin Ahmed Contractor and Suresh Basavaraj Arakera*
and Suresh Basavaraj Arakera*
Department of Applied Genetics, Molecular Medicine and Microbial Genetics Laboratory, Karnatak University, Dharwad, Karnataka, India.
Corresponding Author E-mail: drsbarakera@gmail.com
ABSTRACT: Incidences of methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant (MDR) staphylococci are rising globally, prompting the need to understand human exposure routes, including water sources. This study aimed to analyse water samples from different sources and locations in North Karnataka over a six-month period (November 2021 to April 2022) to determine the prevalence and antibiotic susceptibility of staphylococcal isolates. Water samples were collected using standard microbiological techniques and analysed. Staphylococci were detected in 35.5% (55/155) of the samples and identified using phenotypic tests such as Gram stain, catalase test, and growth and fermentation on mannitol salt media. Methicillin resistance was assessed via cefoxitin disk diffusion, and the presence of the mecA gene was tested by PCR. Among the 55 isolates, 23.6% were resistant to cefoxitin and considered methicillin-resistant, while 36.4% carried the mecA gene. Antibiogram results showed the highest susceptibility to gentamicin (100%) and the lowest to penicillin (12.7%) and oxacillin (1.8%). The nuc gene, encoding thermonuclease, was present in 20% (11/55) of the isolates. Multiple antibiotic resistance (MAR) indices ranged from 0.08 to 0.67, with most staphylococci resistant to at least two antibiotics, and 54.55% (30/55) were MDR. These findings highlight the importance of water, sanitation, and hygiene (WASH) initiatives in reducing the spread of antimicrobial resistance in environmental bacteria.
KEYWORDS: CA-MRSA; MAR index; mecA; nuc; Staphylococci
| Copy the following to cite this article: Contractor S. S. A, Arakera S. B. Antibiotic Susceptibility and Methicillin Resistance in Staphylococcal Isolates from Water Samples in Dharwad and Surrounding Districts of North Karnataka. Biotech Res Asia 2025;22(1). |
| Copy the following to cite this URL: Contractor S. S. A, Arakera S. B. Antibiotic Susceptibility and Methicillin Resistance in Staphylococcal Isolates from Water Samples in Dharwad and Surrounding Districts of North Karnataka. Biotech Res Asia 2025;22(1). Available from: https://bit.ly/41QFB6R |
Introduction
Staphylococcus is a common bacterium found as a commensal in humans and livestock.1,2 Often opportunistic, it usually causes infections of the skin and soft tissue and, in extreme cases, species such as Staphylococcus aureus, can cause endocarditis, osteomyelitis, pneumonia, and septicemia.3 S. aureus is also the primary pathogen for mastitis in cattle1. It can survive adverse environmental conditions such as sunlight and dehydration.1 Drug-resistant variants of this Gram-positive bacterium have emerged as major pathogens among clinical isolates worldwide, posing significant challenges in patient treatment. Based on the global morbidity and mortality rates due to methicillin-resistant S. aureus (MRSA), the World Health Organization (WHO) has categorized it as a ‘serious threat’ pathogen on its 2024 Bacterial Priority Pathogens List.4 MRSA strains are categorized as HA-MRSA, LA-MRSA, and CA-MRSA based on their origin and association (hospital, livestock, or community).
Formerly mostly found in hospitals, MRSA has recently spread significantly among individuals without risk factors or healthcare exposure and has become endemic in India.5 Globally, CA-MRSA strains have proliferated among the general public, affecting both those with and without hospital exposure, and are found in environmental samples such as water, animals, and foods of animal origins. These strains can cause even fatal illnesses, and the transmission of resistance genes from environmental bacteria to human pathogens is a major threat.6 The incidence of CA-MRSA isolates is reportedly on the rise in India.7 The inefficiency of treatment plants is turning the wastewater system into a hotspot for antibiotic-resistant bacteria and genes.5
In staphylococci, methicillin resistance is due to methicillin-hydrolyzing β-lactamase and an altered penicillin-binding protein, PBP2a.8 This 76 kDa protein, encoded by the mecA gene, is situated on the staphylococcal cassette chromosome mec (SCCmec). The altered protein has reduced affinity towards beta-lactam antibiotics in methicillin-resistant strains of staphylococci.9 The acquisition of this gene by sensitive variants of staphylococci leads to the spread of resistance.8
Some strains of the staphylococci produce an extracellular thermonuclease enzyme coded by the nuc gene.10 This 17 kDa protein is an endonuclease that degrades both DNA and RNA, and its enzymatic activity can resist 100oC for at least 1 hour.11 This protein is one of the important virulence markers and adds to the pathogenicity of the bacteria.12
One of the major global threats to the public health is antibiotic resistance, and the emergence of multidrug-resistant (MDR) pathogens poses serious problems in the effective treatment of infectious diseases, causing more deaths than cancer and road accidents combined.13 The alarming rise in antibiotic resistance in India is driven by several factors, including a large, dense population, significant infectious disease burden, high rates of antibiotic consumption due to overprescribing, easy availability of over-the-counter antibiotics, environmental contamination from pharmaceutical industrial effluents, and widespread use of antibiotics in veterinary and agricultural practices.14,15 India leads the global market in antibiotic consumption for human use, with an annual consumption of 12.9 x 109 units.16 Surveillance is vital for detecting MDR organisms, tracking epidemiologic trends, and assessing treatment effectiveness.
Staphylococcus has the ability to adapt and develop resistance to several antibiotics and has been extensively studied in clinical settings.17 However, the prevalence and resistance patterns of Staphylococcus in non-clinical environmental sources, such as water bodies, have not been thoroughly investigated, particularly in North Karnataka, India. While S. aureus is a major pathogen among staphylococci species, recent findings, indicate that the coagulase-negative staphylococci (CoNS), are emerging as stronger pathogens, exhibiting methicillin resistance nearly twice that of S. aureus.18 Therefore, this study examines the prevalence and antibiogram profiles of staphylococcal isolates from water samples collected in and around Dharwad city, North Karnataka.
Materials and methods
Sampling sites and sample collection
The sampling sites were selected using a random sampling method. Water samples were collected from sources such as sewage, ponds, lakes, and rivers over a six-month period (November 2021 to April 2022) from different locations in Dharwad and the surrounding districts of North Karnataka. A total of 155 water samples were collected and screened for staphylococci. Samples were collected in sterile falcon tubes and brought to the laboratory the same day for further processing. For distant locations, samples were inoculated in mannitol salt broth (MSB) at the time of collection and brought to the laboratory within 24 – 48 hours.19
Isolation of staphylococcal isolates
Water samples were enriched before isolating staphylococci. For the enrichment, 1 ml of water sample was added to 10 ml of MSB and incubated overnight at 37oC. The enriched broth was streaked onto mannitol salt agar (MSA) plates, followed by overnight incubation at 37oC. Mannitol-fermenting colonies (yellow) from the MSA plates were transferred to a fresh MSA plate and incubated overnight at 37°C. Round golden yellow colonies with smooth, shining surface and 2-3 mm in diameter were further subjected to Gram staining and catalase testing.19 Mannitol-fermenting, catalase-positive, and Gram-positive cocci present in clusters were identified as staphylococci.20 Purified isolates were stored as stabs in nutrient agar media at 4oC for further characterization and at -20oC in 70% glycerol for long-term storage.
Antibiotic susceptibility testing
This was conducted using the standard Kirby-Bauer disk diffusion method, with results compared to CLSI breakpoints.21 The isolates were tested against 12 different antibiotics (Hi-Media Laboratories Pvt. Ltd.): penicillin (1 U), oxacillin (1 µg), cefoxitin (30 µg), ciprofloxacin (5 µg), erythromycin (15 µg), clindamycin (2 µg), gentamicin (10 µg), linezolid (30 µg), tetracycline (30 µg), rifampicin (5 µg), teicoplanin (30 µg), and chloramphenicol (15 µg). This panel used in routine sensitivity testing is supported by the CLSI guidelines.21 Briefly, an inoculum was prepared by dispersing 2-3 identical colonies followed by incubation until a turbidity of 0.5 McFarland was reached. Using a cotton swab, the inoculum was spread uniformly over MHA plates. Antibiotic discs were placed on the plates, followed by overnight incubation at 37°C. The zones of inhibition were measured, and the results were interpreted according to CLSI guidelines as sensitive, intermediate and resistant.21 Isolates rated as intermediate in antibiotic susceptibility were grouped with the sensitive category, as they can still be treated with elevated doses of antibiotics.22 The Multiple Antibiotic Resistance (MAR) indices were calculated by dividing the number of antibiotics the isolate is resistant to by the total number of antibiotics tested.23
DNA extraction
Bacterial DNA was isolated using the boil lysis method.24 Briefly, 3-4 similar isolated colonies were mixed and boiled in 100 µl of nanopure water at 95oC for 10 minutes. The mixture was cooled and centrifuged at 10,000 rpm for 5 minutes. The supernatant was transferred to a fresh tube and used as a template for gene amplification.
Polymerase chain reaction (PCR)
DNA from the isolates was subjected to multiplex PCR for detection of the thermonuclease (nuc) gene and methicillin resistance (mecA) gene using published primers. Primer sequences were: nucF (5’GGC ATA TGT ATG GCA ATT GTT T3’), nucR (5’ ATA CGC TAA GCC ACG TCC AT3’)12; mecAF (5’GTA GAA ATG ACT GAA CGT CCG ATA A3’), mecAR (5’CCA ATT CCA CAT TGT TTC GGT CTA A3’)25. Primers were synthesized at Eurofins Genomics India Pvt. Ltd. The 25 µl of PCR reaction mixture consisted of 2.5 µl of PCR amplification buffer (10X), 2.5 µl MgCl2 (25 mM), 2.0 µl dNTPs (2 mM), 0.2 µl Taq DNA Polymerase (5U/µl), 1.25 µl of each primer (10 mM), 1.25 µl lysate and 11.55 µl of PCR-grade nanopure water.
PCR amplification was performed using an automated thermal cycler (Eppendorf MC nexus gradient, Flexlid) with the following conditions: initial denaturation at 95°C for 2 minutes; 35 cycles of 95°C for 30 seconds, 62°C for 30 seconds and 72°C for 45 seconds; final extension at 72°C for 10 minutes. Staphylococcus aureus NCIM 5719 (equivalent ATCC BAA-44) was used as a positive control for detecting mecA and nuc genes. To visualize, 5 µl of the PCR product was electrophoresed in 1.5 % agarose, and bands were observed using a UV transilluminator. Amplicons of approximately 489 bp and 310 bp correspond to the presence of nuc and mecA genes, respectively.
The PCR amplified products were sequenced at Biokart, Bengaluru, and analysed using the NCBI BLAST for confirmation. The nuc gene and mecA gene amplicons showed sequence similarities of over 98% and 99%, respectively, with the NCBI database sequences. Additionally, the nuc gene sequence was observed to be distinctive to S. aureus in the database.
Results
In this study, 155 water samples collected and screened from different locations in North Karnataka. From these samples, 55 isolates of staphylococci were recovered, yielding an overall staphylococcal incidence of 35.48%. For convenience, samples from larger water bodies were grouped together. Of the 55 isolates, 18 (32.7%) were from sewage, 23 (41.8%) from lakes and rivers, and 14 (25.5%) from ponds.
The highest antibiotic resistance among the isolates was observed for oxacillin (54/55, 98.2%) followed by penicillin (48/55, 87.3%), erythromycin (26/55, 47.3%), cefoxitin (13/55, 23.6%), clindamycin (8/55, 14.5%), rifampicin (7/55, 12.7%), teicoplanin (4/55, 7.3%), tetracycline (4/55, 7.3%) and linezolid (3/55, 5.5%). Antibiotic resistance was lowest for ciprofloxacin (1/55, 1.8%) and chloramphenicol (1/55, 1.8%), with no resistance observed for gentamicin. The antibiotic susceptibility pattern is represented in Gra. 1.
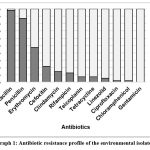 |
Graph 1: Antibiotic resistance profile of the environmental isolates
|
Out of the 55 isolates, 30 (54.55%) were considered as multi- drug resistant (MDR) according to the criteria stated by Magiorakos et al.23 However, none exhibited extensive drug resistance (XDR) or pan-drug resistance (PDR) according to the Centers for Disease Control and Prevention (CDC) definitions. The MAR indices ranged from 0.08 and 0.67, with a mean of 0.26, and both median and modal values were 0.16, indicating that most isolates were resistant to at least two antibiotics. Gra. 2. represents the frequency of resistant staphylococci for the number of antibiotics.
A one-way analysis of variance (ANOVA) was conducted to determine if there were significant differences in the mean MAR values among the four groups (Lake, Pond, River, and Sewage). The analysis revealed no statistically significant differences in the mean MAR values across the four groups at the 0.05 significance level, [F= 1.850, F crit = 2.798, p = 0.1508], indicating all samples contained MDR isolates without any significant difference.
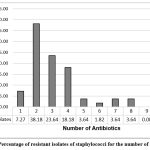 |
Graph 2: Percentage of resistant isolates of staphylococci for the number of antibiotics
|
Out of the 55 isolates, 13 (23.6%) were identified as methicillin-resistant using cefoxitin sensitivity testing. The mecA gene PCR was positive in 20 (36.4%) isolates, while 35 isolates were negative for mecA. Among the cefoxitin-resistant isolates, four were negative for the mecA gene, while 11 isolates with the mecA gene were sensitive to cefoxitin. Given that the cefoxitin disc diffusion method is the standard practice in most laboratories, the prevalence of methicillin resistance in our study was 13 out of 55 (23.6%). Table 1 presents MRSA detection results by phenotypic and genotypic methods.
Table 1: Frequency of methicillin-resistant staphylococci by phenotypic and genotypic tests
| Test | Methicillin Resistance | Percentage |
| Cefoxitin Disc diffusion | 13 | (23.6%) |
| mecA gene (PCR) | 20 | (36.4%) |
In this study, we explored the nuc gene as an indicator of S. aureus pathogenicity and included it in our species confirmation tests. Our findings showed that 11 out of 55 staphylococcal isolates (20%) carried the nuc gene. The presence of thermonuclease is indicative of their potential pathogenic nature.11
Discussion
This study investigated the dissemination of antibiotic resistance among staphylococci isolated from various surface water sources in and around Dharwad city, North Karnataka, India. We recorded antibiotic susceptibility and conducted comparative analysis for methicillin resistance using both phenotypic and genotypic tests. Similar studies in India and other countries have reported MDR staphylococci in diverse water samples.1,5,17, 26
The incidence of water-related diseases in India is high, with nearly 3.7 million cases reported annually.27 This is due to poor waste management, human and animal interventions, and inadequate wastewater treatment, leading to pollution of water bodies and becoming pathogen breeding grounds.17 Hospital effluents, disposal of unused medicines, and untreated wastewater from slaughterhouses contribute to MDR bacterial populations in the environment.6 A 2018 study found that about 30% of the Indian population lacks proper latrine facilities, leading to open defecation.28 Climatic changes and heavy rains cause the mixing up of sewage water, thereby increasing health risks.27
The detection of staphylococci in water sources is linked to human activities and the presence of domestic animals and livestock.2 Infected animals serve as reservoirs of MRSA.1 The prophylactic use of antimicrobials in agriculture, aquaculture, animal husbandry, poultry, and pig farming has led to a rise in MDR strains of staphylococci in the environment.29
Some researchers found a strong association between S. aureus and the use of the nuc gene for its rapid identification. However, it is not highly specific, as other species of staphylococci, streptococci, and possibly other bacteria may mimic the enzymatic activity produced by the thermonucleases.11 Our study reported the presence of nuc gene in 11 out of 55 (20%) staphylococcal isolates, indicating greater thermal stability and pathogenicity.11 Another study conducted by our team during the same period, involving 250 clinical isolates of staphylococci found the nuc gene in 60.8% of S. aureus and 17.2% of the CoNS isolates.30 Other researchers reported its presence in 80.2%31 and 50%12 of S. aureus isolates, respectively.
The prevalence of methicillin resistance in our study was found to be 23.6%. This finding aligns with other research conducted in India, which reported methicillin resistance prevalence of 25% in Delhi NCR,5 22.62% in Jalandhar, Punjab,32 and 19.09% in Assam,33 in studies focused on antimicrobial resistance (AMR) in water samples for staphylococcal isolates. Internationally, methicillin resistance prevalence has been reported as follows: 36.7% in Brazil,17 16.7% in Nigeria,34 97.5% in South Africa,35 and 27% in USA.36
According to the Indian Council of Medical Research’s 2023 antimicrobial resistance surveillance report, the prevalence of MRSA in clinical isolates across India varied significantly, ranging from 25% to 85% among the different regional centers involved in the study.30,37 Between 2015 and 2019, the mean frequency of MRSA was as follows in various regions of India: North: 41%, East: 43%, West: 33%, South: 34%, Central: 36%, and Northeast: 40%.38 Internationally, MRSA has the highest prevalence (60-80%) in the Middle East and North African countries, while in sub-Saharan Africa and several European countries have reported the least prevalence (< 5%).39
Presently, most staphylococci show high resistance to penicillin and ampicillin.1 Our study observed similar resistance patterns, with high resistance to erythromycin (47.3%). This can be attributed to selection pressure due to the excessive use of these commonly used antibiotics not just by human and veterinary clinical practitioners but also in poultry and agriculture as a prophylactic treatment. Interestingly, low resistance to chloramphenicol and ciprofloxacin, and no resistance to gentamicin, suggests these antibiotics remain effective against majority of the environmental isolates. This finding is in agreement with other studies.29,40 This is particularly relevant considering the global concern over the decreasing effectiveness of numerous antibiotics.
In our study, 98.2% of isolates were resistant to oxacillin. Some researchers have even reported 100% oxacillin resistance in environmental isolates.26 Due to high specificity and sensitivity, the CLSI have recommended cefoxitin over oxacillin in the phenotypic detection of methicillin resistance in staphylococci.21,41 However, phenotypic sensitivity might not accurately reflect the true nature of the organism, as it can be influenced by external factors such as inoculum concentration, salt concentration in the media, incubation time, and temperature, among others.42 OS-MRS (oxacillin-susceptible methicillin resistant staphylococci) is a subpopulation of MRS that, despite carrying the mecA gene, appears susceptible to routine phenotypic tests like cefoxitin disc diffusion or oxacillin screen agar, potentially leading to its misidentification as methicillin susceptible staphylococci43 this could be due to frameshift mutation, gene regulation, modification of cell wall, heterogenous resistance.31,44 In our current study, we identified 11 (20%) instances of OS-MRS. Previous studies have reported rates of 2%,43 7.09%,18 and 7.2%.30
Isolates phenotypically detected as methicillin-resistant but lacking the mecA gene by PCR might result from altered expression of penicillin-binding proteins (PBPs) due to gene mutation, β-lactamase overproduction leading to borderline oxacillin resistance staphylococci (BORS), or the potential involvement of alternative resistance mechanisms, like efflux pumps or target site modifications.21,29 Recently, the mecC gene has been identified as another factor contributing to methicillin resistance, with a 60% homology to the mecA gene.43 However, we did not test for the presence of the mecC gene in our isolates. The incidence of BORS/ORS (oxacillin-resistant staphylococci) in our study was 7.2%, other researchers have reported rates of 2.4%,18 6%,45 12.8%,30 and 25.5%.46
The global spread of MDR staphylococci is concerning. An important observation from this study is the slight elevation in MAR indices, with a value of 0.26. MAR indices above 0.25 suggest higher and recurrent antibiotic exposure environments.23 Other studies have reported MAR value ranging from 0.38–0.52,32 0.435.34 Rajput et al.5 reported 60.86% MDR strains of staphylococci in their study.
In our clinical isolates study, 86.4% showed methicillin resistance by cefoxitin, and 80.8% by the presence of mecA. MAR indices ranged from 0.12 to 0.65 in S. aureus and 0.06 to 0.71 in CoNS. The average MAR values in S. aureus and coagulase-negative staphylococci (CoNS) were 0.42 and 0.44, indicating resistance to seven or more antibiotics.30 This highlights higher and more frequent antibiotic resistance in clinical isolates compared to environmental isolates. However, MAR values above 0.25 still indicate a rising AMR threat among environmental isolates. This issue requires timely attention and adequate action to curb the rise of AMR in environmental isolates.
The broader implications of our findings underscore the increasing prevalence of AMR globally, driven by antibiotics misuse in human and animal healthcare, inadequate wastewater treatment, and the improper pharmaceutical disposal. The emergence of ‘superbugs’ and the corresponding rise in healthcare costs and treatment complexities represent a substantial burden on public health systems worldwide.47 The situation is further complicated by the lack of strong surveillance data in many regions, including India, where environmental AMR remains underreported.
To address the escalating threat of antimicrobial resistance, global initiatives such as the World Health Organization’s ‘One Health’ approach, Global Action Plan, Antibiotic Stewardship Programme, and the Global Antimicrobial Resistance and Use Surveillance System (GLASS) play a crucial role.13 These initiatives advocate for coordinated efforts across human, animal, and environmental health sectors to tackle AMR, monitor the spread of drug resistance, and improve patient care by reducing irrational antibiotic use.
In India, the National Action Plan for AMR has been introduced to regulate the use of antimicrobials, including prohibiting the use of last-resort antibiotics in poultry feed and farming. The National Centre for Disease Control and the Indian Council of Medical Research (ICMR) monitor AMR through the AMR Surveillance and Research Network (AMRSN). This network combats antibiotic misuse in hospitals and monitors AMR status in clinical isolates through regular surveillance of 30 tertiary care hospitals selected across the nation by ICMR’s Antimicrobial Stewardship Program (AMSP).15 ICMR raises awareness through initiatives in educational institutes and conducts workshops for microbiologists and healthcare workers. Emphasis is laid on all stakeholders, including clinicians, farmers, public, and drug companies, to jointly address antibiotic resistance and curb its growing menace.48
Additionally, the WHO has introduced the WASH program in India and other countries, aiming to provide clean drinking water, better sanitation, and improved hygiene practices. Key initiatives under this program in India include the Swachh Bharat Mission and the Jal Jeevan Mission.28
Conclusion
The present study was driven by the scarcity of data on antimicrobial resistance in environmental isolates of staphylococci. Our study contributes to understanding the AMR burden in these isolates and emphasizes the need to address this complex challenge by adopting integrated approaches. These approaches include raising public awareness about the rational use and disposal of pharmaceutical products and ensuring adequate wastewater treatment to avoid the contamination of freshwater and other water bodies. Further research is required to inspect the spread of drug resistance in other environmental samples, such as food and meat, and to develop effective interventions to prevent the dissemination of resistant pathogens in the environment. Such initiative can significantly prolong the efficacy of antibiotics in clinical applications.
Acknowledgement
The authors express their gratitude to the Department of Applied Genetics, Karnatak University, Dharwad, for providing the necessary facilities required to conduct the research experiments.
Funding Sources
The authors declare that they received financial assistance from Karnatak University for funding this work through the University Research Scholarship (Grant No: KU/MOBC/URS/2021/660 dated 01/10/2021).
Conflict of Interest
The authors have no financial and non-financial conflicts of interest to disclose.
Data Availability Statement
This statement does not apply to this article
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not Applicable
Author Contributions
Shafa Contractor: Data collection, Methodology, Analysis, Funding Acquisition, Writing- Original Draft & Editing.
Suresh Arakera: Conceptualization, Supervision, Writing- Review & Finalized the manuscript.
Both the authors mentioned have significantly and directly contributed intellectually to the project and have given their approval for its publication.
References
- Algammal A.M., Hetta H.F., Elkelish A., et al. Methicillin-Resistant Staphylococcus aureus (MRSA): One Health Perspective Approach to the Bacterium Epidemiology, Virulence Factors, Antibiotic-Resistance, and Zoonotic Impact. Infect Drug Resist. 2020;13:3255-3265.
CrossRef - Goodwin K.D., McNay M., Cao Y., Ebentier D., Madison M., Griffith J.F. A multi-beach study of Staphylococcus aureus, MRSA, and enterococci in seawater and beach sand. Water Res. 2012;46(13):4195-4207.
CrossRef - Tong S.Y.C., Davis J.S., Eichenberger E., Holland T.L., Fowler V.G. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clin Microbiol Rev. 2015;28(3):603-661.
CrossRef - WHO BPP List. Bacterial Pathogens of Public Health Importance to Guide Research, Development and Strategies to Prevent and Control Antimicrobial Resistance.; 2024.
- Rajput S., Mitra S., Mondal A.H., Kumari H., Mukhopadhyay K. Prevalence and molecular characterization of multidrug-resistant coagulase negative staphylococci from urban wastewater in Delhi-NCR, India. Arch Microbiol. 2024;206(10):399.
CrossRef - Kamatham S., Seeralan M., Sekar U., Kuppusamy S. Antimicrobial Resistance Profiling of Bacterial Isolates from Wastewater and Environmental Samples Collected from Pharmaceutical Industries in South India. Published online April 26, 2024.
CrossRef - Joshi S., Ray P., Manchanda V., et al. Methicillin resistant Staphylococcus aureus (MRSA) in India: Prevalence & susceptibility pattern. Indian J Med Res. 2013;137(2):363-369.
- Unnikrishnan M.K., Eldo P.A., Anburaj S.E., Chandra P., Rajesh V. For whom the bell tolls? Methicillin-resistant Staphylococcus aureus infections in India. J Appl Pharm Sci. Published online 2023.
CrossRef - Chambers H.F. Methicillin resistance in staphylococci: molecular and biochemical basis and clinical implications. Clin Microbiol Rev. 1997;10(4):781-791.
CrossRef - Sahebnasagh R., Saderi H., Owlia P. The Prevalence of Resistance to Methicillin in Staphylococcus aureus Strains Isolated from Patients by PCR Method for Detection of mecA and nuc Genes. Iran J Public Health. 2014;43(1):84-92.
- Brakstad O.G, Aasbakk K., Maeland J.A. Detection of Staphylococcus aureus by polymerase chain reaction amplification of the nuc gene. J Clin Microbiol. 1992;30(7):1654-1660.
CrossRef - Adei̇Za S.S., Onaolapo J.A., Olayinka B.O. Genetic Profiling of Methicillin-resistant Staphylococcus aureus in An African Hospital by Multiplex-PCR. J Microbiol Infect Dis. 2020:144-153.
CrossRef - O’Neill J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Review on Antimicrobial Resistance; 2016.
- Taneja N., Sharma M. Antimicrobial resistance in the environment: The Indian scenario. Indian J Med Res. 2019;149(2):119.
CrossRef - Singh V.P., Jha D., Rehman B.U., Dhayal V.S., Dhar M.S., Sharma N. A mini-review on the burden of antimicrobial resistance and its regulation across one health sectors in India. J Agric Food Res. 2024;15:100973.
CrossRef - Chauhan J., Chakraverty R., Pathan S. Antimicrobial stewardship program activities in India: an appraisal. Int J Basic Clin Pharmacol. 2022;11(6):676.
CrossRef - Santos G.A.C., Dropa M., Rocha S.M., Peternella F.A.S., Razzolini M.T.P. Staphylococcus aureus and methicillin-resistant Staphylococcus aureus (MRSA) in drinking water fountains in urban parks. J Water Health. 2020;18(5):654-664.
CrossRef - Rajkumar S., Sistla S., Manoharan M., et al. Prevalence and Genetic Mechanisms of Antimicrobial Resistance in Staphylococcus Species: A Multicentre Report of the Indian Council of Medical Research Antimicrobial Resistance Surveillance Network. Indian J Med Microbiol. 2017;35(1):53-60.
CrossRef - Clesceri L., Greenberg A., Eaton A. Standard Methods for the Examination of Water and Wastewater. 21st ed. Federation WE, Aph Association. Standard methods for the examination of water and wastewater.; 2005.
- Ananthanarayan R. Ananthanarayan and Paniker’s Textbook of Microbiology. 7th ed. Orient Blackswan; 2006.
- Weinstein M.P. M100-Performance Standards for Antimicrobial Susceptibility Testing, 28th Edition. CLINICAL AND LABORATORY; 2018.
- Rodloff A., Bauer T., Ewig S., Kujath P., Müller E. Susceptible, Intermediate, and Resistant – The Intensity of Antibiotic Action. Dtsch Ärztebl Int. 2008:105(39): 657-62.
CrossRef - Magiorakos A.P., Srinivasan A., Carey R.B., et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268-281.
CrossRef - Dashti A.A., Jadaon M.M., Abdulsamad A.M., Dashti H.M.. Heat Treatment of Bacteria: A Simple Method of DNA Extraction for Molecular Techniques. KUWAIT Med J. 2009.
- Zhang K., Sparling J., Chow B.L., et al. New Quadriplex PCR Assay for Detection of Methicillin and Mupirocin Resistance and Simultaneous Discrimination of Staphylococcus aureus from Coagulase-Negative Staphylococci. J Clin Microbiol. 2004;42(11):4947-4955.
CrossRef - Iroha I.R. In vitro antibiogram of multidrug resistant bacteria isolated from Ogbete abattoir effluent in Enugu State, Nigeria. Int Res J Public Environ Health. 2016;3(1).
- Sharma M.D., Mishra P., Ali A., et al. Microbial Waterborne Diseases in India: Status, Interventions, and Future Perspectives. Curr Microbiol. 2023;80(12):400.
CrossRef - Vennu V. Drinking water, sanitation, hygiene, and health conditions in India: Findings from the national sample survey. J Fam Med Prim Care. 2024;13(4):1535-1543.
CrossRef - Shivakumaraswamy S., Deekshit V., Vittal R., et al. Phenotypic & genotypic study of antimicrobial profile of bacteria isolates from environmental samples. Indian J Med Res. 2019;149(2):232.
CrossRef - Contractor S.S., Kulkarni R.D., Arakera S.B. Prevalence, Antibiotic Susceptibility Pattern and the Detection of mecA Gene among Staphylococcus spp. Isolates from a Tertiary Care Hospital in North Karnataka. Indian J Microbiol. Published online October 6, 2024.
CrossRef - Sahebnasagh R., Saderi H., Owlia P. The Prevalence of Resistance to Methicillin in Staphylococcus aureus Strains Isolated from Patients by PCR Method for Detection of mecA and nuc Genes. Iran J Public Health. 2014;43(1):84-92.
- Kumar H., Palaha R., Kaur N., et al. Prevalence of multidrug-resistant, coagulase-positive Staphylococcus aureus in nasal carriage, food, wastewater and paper currency in Jalandhar city (north-western), an Indian state of Punjab. Environ Monit Assess. 2015;187(1):4134.
CrossRef - Bhowmik D., Chetri S., Das B.J., Dhar C. D., Bhattacharjee A. Distribution of virulence genes and SCCmec types among methicillin-resistant Staphylococcus aureus of clinical and environmental origin: a study from community of Assam, India. BMC Res Notes. 2021;14(1):58.
CrossRef - Oladipo A.O., Oladipo O.G., Bezuidenhout C.C. Multi-drug resistance traits of methicillin-resistant Staphylococcus aureus and other Staphylococcal species from clinical and environmental sources. J Water Health. 2019;17(6):930-943.
CrossRef - Silva V., Caniça M., Capelo J.L., Igrejas G., Poeta P. Diversity and genetic lineages of environmental staphylococci: a surface water overview. FEMS Microbiol Ecol. 2020;96(12):fiaa191.
CrossRef - Fogarty L.R., Haack S.K., Johnson H.E., Brennan A.K., Isaacs N.M., Spencer C. Staphylococcus aureus and methicillin-resistant S. aureus (MRSA) at ambient freshwater beaches. J Water Health. 2014;13(3):680-692.
CrossRef - National AMR Surveillance Network (NARS-Net) Annual Report 1 January 2023 31 December 2023. Available Online at: National AMR Surveillance Network (NARS-Net) Annual Report 2023: Ministry of Health and Family Welfare (Ncdc. Gov.in); 2024.
- Patil S.S., Suresh K.P., Shinduja R., et al. Prevalence of Methicillin-resistant Staphylococcus aureus in India: A Systematic Review and Meta-analysis. Oman Med J. 2022;37(4):e440-e440.
CrossRef - Naghavi M., Vollset S.E., Ikuta K.S., et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. The Lancet. 2024
- Bharti, Bali P., Minhas N. Isolation and characterization of multi-drug resistant (MDR) and extensively drug resistant (XDR) bacterial pathogens from diverse environmental niches of Shimla, Himachal Pradesh (India). Published online February 3, 2023
CrossRef - Broekema N.M., Van T.T., Monson T.A., Marshall S.A., Warshauer D.M. Comparison of Cefoxitin and Oxacillin Disk Diffusion Methods for Detection of mecA -Mediated Resistance in Staphylococcus aureus in a Large-Scale Study. J Clin Microbiol. 2009;47(1):217-219.
CrossRef - Akcam F.Z., Tinaz G.B., Kaya O., Tigli A., Ture E., Hosoglu S. Evaluation of methicillin resistance by cefoxitin disk diffusion and PBP2a latex agglutination test in mecA-positive Staphylococcus aureus, and comparison of mecA with femA, femB, femX positivities. Microbiol Res. 2009;164(4):400-403.
CrossRef - Nair D., Shashindran N., Kumar A., Vinodh V., Biswas L., Biswas R. Comparison of Phenotypic MRSA Detection Methods with PCR for mecA Gene in the Background of Emergence of Oxacillin-Susceptible MRSA. Microb Drug Resist. 2021;27(9):1190-1194.
CrossRef - Goering R.V., Swartzendruber E.A., Obradovich A.E., Tickler I.A., Tenover F.C. Emergence of Oxacillin Resistance in Stealth Methicillin-Resistant Staphylococcus aureus Due to mecA Sequence Instability. Antimicrob Agents Chemother. 2019;63(8):e00558-19.
CrossRef - Loganathan A., Nachimuthu R. Antibiotic resistance, biofilm forming ability, and clonal profiling of clinical isolates of Staphylococcus aureus from southern and northeastern India. Asian Biomed. 2022;16(4):191-199.
CrossRef - Khorvash F., Mostafaviz K., Mobasheriz S. Frequency of mecA Gene and Borderline Oxacillin Resistant Staphylococcus aureus in Nosocomial Acquired Methicillin Resistance Staphylococcus aureus Infections. Pak J Biol Sci. 2008;11(9):1282-1285.
CrossRef - Salam M.A., Al-Amin M.Y., Salam M.T., et al. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare. 2023;11(13):1946.
CrossRef - Chandy S.J., Michael J.S., Veeraraghavan B., Abraham O.C., Bachhav S.S., Kshirsagar N.A. ICMR programme on Antibiotic Stewardship, Prevention of Infection & Control (ASPIC). Indian J Med Res. 2014;139(2):226-230.
Abbreviations
AMR– Antimicrobial Resistance;
CoNS- Coagulase Negative Staphylococci;
MAR- Multiple Antibiotic Resistance;
MDR– Multidrug-Resistant;
MRS- Methicillin Resistant Staphylococci;
MRSA- Methicillin Resistant Staphylococcus aureus;
WHO- World Health Organization;
MSA– Mannitol Salt Agar

This work is licensed under a Creative Commons Attribution 4.0 International License.



