

How to Cite | Publication History | PlumX Article Matrix
Roua Mohammad Saleh Alkufeid , Mohamed Abdellatif El-Tayeb*
, Shuruq Ahmed Othman Alshabanat, Mshael Mohammed Thabit Bin Madhi
, Noura Saleem Duhaim Aldosari, and Nura Suliman Abdullah Alsakabi
, Mohamed Abdellatif El-Tayeb*
, Shuruq Ahmed Othman Alshabanat, Mshael Mohammed Thabit Bin Madhi
, Noura Saleem Duhaim Aldosari, and Nura Suliman Abdullah Alsakabi
Department of Botany and Microbiology, College of Sciences, King Saud University, Riyadh, Saudi Arabia.
Corresponding Author E-mail:mali5@ksu.edu.sa
ABSTRACT: The widespread use of mobile phones in daily human transactions, especially those related to the medical field, leads to the spread of microbes among different communities. The microbiology student’s mobile phones could harbour various drug-resistant microbes involved in nosocomial infections to the family members. This study aimed to isolate and characterize bacteria from the mobile phones of microbiology students and other students. This cross-sectional study was performed using a random sampling technique. All data were collected using a questionnaire. Sixty samples were obtained from the surface of the mobile phones of 60 volunteers at King Saud University (KSU). Twenty-three (77%) microbiology students used their mobile phones in the toilets, compared to 23 (77%) non-microbiology students. Staphylococcus is the most prevalent organism followed by Bacillus. The isolated S. aureus was Ampicillin and polymyxin B resistant. It was intermediate against the tested Sulfamethoxazole and Bacitracin. S. aureus isolated from microbiology and non-microbiology students showed no antibiotic sensitivity changes. S. epidermidis showed resistance against Polymyxin B and exhibited an intermediate response against sulfamethoxazole and bacitracin. Bacillus sp. exhibited resistance against Erythromycin. The prevalence of bacteria was higher in microbiology students than in non-microbiology students. The mobile phones of microbiology students were contaminated with clinical pathogens. Therefore, suitable methods should be developed to prevent the outbreak of nosocomial pathogens from the laboratories.
KEYWORDS: Bacillus sp; Bacteria; Drug-resistance; Mobile phone; Transmission
| Copy the following to cite this article: Alkufeid R. M. S, El-Tayeb M. A, Alshabanat S. A. O, Madhi M. M. T. B, Aldosari N. S. D, Alsakabi N. S. A. Prevalence of Drug-Resistant Nosocomial Pathogenic Bacterial Strains Isolated from Mobile Phones: A Cross-Sectional Study Between Microbiology Students and Other Disciplines. Biotech Res Asia 2025;22(1). |
| Copy the following to cite this URL: Alkufeid R. M. S, El-Tayeb M. A, Alshabanat S. A. O, Madhi M. M. T. B, Aldosari N. S. D, Alsakabi N. S. A. Prevalence of Drug-Resistant Nosocomial Pathogenic Bacterial Strains Isolated from Mobile Phones: A Cross-Sectional Study Between Microbiology Students and Other Disciplines. Biotech Res Asia 2025;22(1). Available from: https://bit.ly/4kWs19e |
Introduction
Mobile phones serve as breeding grounds, making them perfect platforms for disease distribution by simple microbial dispersal in the environment, public spaces, and the workplace, or through self-inoculation through contact with one’s phone and face.1 It has been shown that healthcare personnel’s cell phones can act as nosocomial infection reservoirs.2 One of the most necessary accessories for social and professional life nowadays is mobile phones (MPs). Despite their many advantages, MPs provide an excellent habitat for infectious diseases inside communities.3 During their internships at hospitals or clinical laboratories, health sciences majors’ students and laboratory personnel utilize their MPs to snap images during their practices, answer calls, text messages, or access material from their field of expertise.4 Cross-contamination is more likely when MPs are used often in a variety of locations, particularly if there are no standard safety procedures or hygiene safeguards in place; should infections be found on MPs’ surface, they may spread to the user’s skin, other surfaces, or food, where they may thrive and multiplicate. Therefore, the recent research on MPs has mostly focused on nosocomial pathogen transmission and hospital-acquired illnesses.5-6
The use of technology in aiding students’ learning has grown significantly in recent years since it appears that technology will play a major part in higher education. The utilization of technology and innovations in Education 4.0 is anticipated to offer substantial benefits to higher education establishments in Malaysia. With the advent of new technologies like paper-thin cellphones, AI, and QR codes, kids will have more time to study and develop new abilities.3 Although hand-washing helps humans lower the microbial burdens on their hands, people use their mobile phones without thinking about disinfection since they are exposed to more environmental factors.2 Mobile phones frequently come into close contact with infected human body parts during phone conversations, including the hands, mouth, nose, and ears. According to a recent assessment, roughly 90.7% of Nigeria’s population, or 205.4 million cellular mobile connections, were active as of early 2024.7 Mobile phones serve as breeding grounds, making them perfect platforms for disease spreading by simple microbial dispersal in the environment, public spaces, or the workplace, or through self-inoculation through contact with one’s phone and face.2
While several microbes have been linked to mobile phone contamination, the most significant infectious agent to be isolated from mobile phones is the skin colonizer Staphylococcus aureus (S. aureus).8 Many previous studies have indicated that mobile phones were contaminated with S. aureus in healthcare workers and medical students. 9
The number of mobile phone users in Saudi Arabia increased from 2015 to 2017. In 2015, it was estimated about 19.42 million phone users and this number increased in 2016 (20.38 million). In 2017, the number reached 21.18 million.10 In India, about 287 million people use mobile phones and this revealed that about 85% of all telecommunication is performed using cell phones.11 Healthcare workers use a mobile phone in a hospital environment under various circumstances. With all the achievements and benefits of mobile phones, it is considered a carrier of several microbes.12 One of the studies revealed that 42% of mobile phones carried by healthcare workers and only 18% of the general public were contaminated with one or more microorganisms.13 Micro-flora on mobile phones of Healthcare workers may vary widely based on the exposure to the healthcare environment, and susceptibility to different antibiotics than non-healthcare workers.14 The constant handling of mobile phones by users in hospitals and microbiology laboratories makes it a hot spot for microbial healthcare-associated infection transmission. This is associated with the skin due to the moisture and optimum temperature of the human body our palms.15 These factors and the heat generated by mobile phones contribute to harboring bacteria on the device at alarming levels.12 It was previously reported that >90% of healthcare workers’ mobile phones were contaminated with microorganisms and >14% of them carried pathogenic bacteria that commonly cause nosocomial infections.16 The resistance of clinically significant bacterial pathogens to common antimicrobial therapies and the emergence of multidrug-resistant bacteria are increasing at an alarming rate, and it has become a major problem in the treatment of Gram-positive bacterial infections.17 Antimicrobial resistance in bacterial pathogens has become a worldwide challenge associated with high morbidity and mortality.18 People rarely disinfect mobile phones and remain unclean at almost all times.19 Microbiology students are working in bacteriology labs, virology labs, mycology labs, and molecular genetics labs, most of them have mobile phones while working, hence posing a serious threat to microbial contamination. The mobile phones used by microbiology students often become carriers and may serve as vectors and spread microorganisms.14 Colonized microorganisms on the devices of microbiology students may be transmitted to other family members or students, who do not have direct contact with their mobile phones, the transmitted pathogenic organisms affect the health of humans, especially immunocompromised individuals.14 The continuous handling of mobile phones by users in hospitals or microbiology laboratories by doctors, or students, makes it a critical point for the transmission of pathogenic bacteria, that colonized in the mobile phone may be transmitted to other individuals, those pathogenic organisms affect the individuals, especially immunocompromised cases and if the organisms were drug-resistant, the situation becomes more alarming as it becomes almost impossible to treat because of the limited drug options available. 2 There are germs on cell phones that can spread to patients and cause sepsis.20 The microbiology students working in the laboratories have contact with many types of pathogenic bacteria.2 The present study aimed to investigate the presence and the rate of antibiotic resistance of pathogenic bacteria on mobile phones that microbiology students frequently use compared to other students.
Materials and methods
Experimental design
This study was performed at the Department of Microbiology, King Saud University (KSU), Riyadh, Saudi Arabia. Sixty samples were collected from the mobile phones of the microbiology student volunteers (n = 30) and other department students (n = 30) based on accredited questionnaires for data collection.16 The questionnaire included variables such as the use of mobile phones in toilets, the use of disinfectants to clean the surface of the mobile phones, and the use of mobile phones in the laboratory.
Characterization of bacteria
A total of sixty sample were collected from mobile phone using sterile cotton swab with brain heart infusion broth (Thermo Fisher Scientific, USA) for 2 hours at 37°C, followed by 10-fold serial dilution on 0.9% sterile normal saline.21 Then 0.1mL of an appropriated dilution (103) was inoculated into nutrient agar (Oxoid, UK) and inoculated at 37°C overnight. The pure bacterial isolates were obtained after repeated plating techniques on nutrient agar. The isolated strains were identified using colonial morphology and biochemical tests. Moreover, the identification of isolated strains was confirmed using an automated system Microscan. Two Microscan devices were used to identify bacteria. The instruments used were, “The Siemens MicroScan® Walk Away 96si” from “King Saud Chest Hospital bacteriology laboratory” and Beckman Coulter Microscan® Walk Away from King Khalid University Hospital (Model No.:3251-2654A).22-23
Antibiotic susceptibility analysis
The antibiotic susceptibility test was performed as described previously with minor modifications. An antibiotic sensitivity test was performed using multiple antibiotic discs. The bacterial suspension of each bacterium was in a concentration equivalent to McFarland 0.5 and was applied on Mueller-Hinton agar with 4% NaCl. The inhibition zone diameters were measured and interpreted according to the Clinical and Laboratory Standards Institute (CLSI). The organisms were classified as resistant (>18 mm), intermediate (≤ 18 mm), and susceptible (≥ 21 mm).24
Results
Determination of bacteria on the surface of mobile phones
Out of 60 mobile phones, bacterial growth was obtained in 56 (93%) mobile phones. In this study, 90% of mobile phone microbiology students (n=27) and 96% of students from other categories (n=29) carried microorganisms in their mobile phones. The variation between microbiology and non-microbiology students was not statistically significant (p>0.05) (Fig 1).
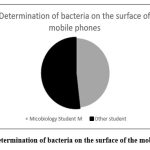 |
Figure 1: Determination of bacteria on the surface of the mobile phones |
Questionnaire analysis
Sixty samples were obtained from the surface of the mobile phones of 60 volunteers at King Saud University (KSU). A total of 23 (77%) microbiology students used their mobile phones in the toilets, while 7(23%) did not use them in the toilets. About 21 (70%) non-microbiology students used their mobile phones in the toilets. About 9 (30%) microbiology students used disinfectants to clean their mobile phones regularly, while 21(70%) did not clean their mobile phones during the study period. Only 7(23%) non-microbiology students used disinfectant to clean mobile phones. In the microbiology lab, 90% (n = 27) of the microbiology students followed standard operating procedures and did not use mobile phones and only 3 persons used mobile phones Fig 2.
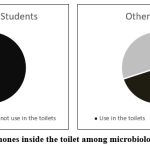 |
Figure 2: Use mobile phones inside the toilet among microbiology students and others. |
Analysis of cultural characteristics of bacteria
The morphological properties of isolated drug-resistant bacteria were determined. The margin of the isolate was undulate, entire, and lobate. The elevation of the isolated colonies is depicted in (Table 1). Red and yellow pigments were observed.
Table 1: Characteristics of bacterial colonies on nutrient agar medium
| Sample\ characteristics | Margin | Elevation | Pigmentation | Size | Shape |
| 25-M* | Entire | Raised | Cream | Tiny | Circular |
| 4-M | Undulate | Flat | Cream | Large | Irregular |
| 22-M (1) | Undulate | Flat | Cream | Large | Irregular |
| 7-O**(1) | Filiform | Flat | Cream | Tiny | Circular |
| 24-O | Lobate | Raised | Cream | Large | Circular |
| 22-M | Entire | Raised | Cream | Medium | Circular |
| 6-O | Entire | umbonate | Cream | Medium | Circular |
| 2-O | Lobate | Raised | Cream | Medium | Circular |
| 8-M (2) | Undulate | Flat | Cream | Large | Irregular |
| 2-M | Entire | Raised | Cream | Medium | Circular |
| 12-M | Entire | umbonate | Red | Medium | Circular |
| 10-O | Undulate | Raised | Cream | Large | Irregular |
| 17-O | Undulate | Umbonate | Yellow | Tiny | Irregular |
| 9-M | Undulate | Flat | Cream | Large | Irregular |
| 6-M | Entire | Umbonate | Cream | Medium | Circular |
| 11-M | Entire | Convex | Yellow | Tiny | Circular |
| 12-O | Entire | Convex | Yellow | Tiny | Circular |
| 24-M | Entire | Raised | Cream | Medium | Circular |
| 21-O | Undulate | Flat | Cream | Large | Irregular |
*Microbiology students, ** Other students
Morphological features of the bacteria isolated from mobile phones
Most isolated bacteria were Gram-positive; only one organism was a Gram-negative strain (Fig. 3). One actinomycete strain was observed in this study. Most characterized bacteria were rod-shaped bacilli, followed by grape-like cocci, filamentous, and Tetrad shape (Table 2).
Table 2: Morphological characters of the bacteria isolated from the mobile phones of microbiology and other students.
| Sample No. | Shape | Gram staining |
| 2-O** | Bacilli | +*** |
| 12-O | Spirillum | + |
| 7-M* | Bacilli | + |
| 6-O | Grape shape like cocci in clusters | + |
| 22-M (2) | Bacilli | + |
| 10-O | Bacilli | + |
| 2-M | Cocci | + |
| 6-M | Cocci | + |
| 3-O | Bacilli | + |
| 24-M | Filamentous or spirillum | + |
| 21-O | Bacilli | + |
| 17-O | Cocci | -**** |
| 25-M | Long bacilli in chains | + |
| 22-M | bacilli chains | + |
| 24-O | Bacilli | + |
| 9-M | Bacilli | + |
| 3-M | Grape shape like cocci in clusters | + |
| 4-M | Bacilli | + |
| 8-M | Bacilli | + |
| 12-M | Tetrad | + |
*Microbiology students, **Other students, ***Gram positive bacteria. ***** Gram-negative bacteria.
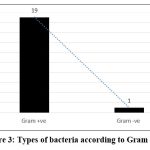 |
Figure 3: Types of bacteria according to Gram stain |
Identification of bacteria from mobile phones using an automated Microscan device
Staphylococcus is the major strain identified in this study and was predominant on the skin surface. So, naturally, mobile phones are exposed to Staphylococcus sp. Staphylococcus aureus was found in three samples, and Staphylococcus schleiferi, and Staphylococcus epidermidis were also detected. Moreover, other bacterial species such as Micrococcus sp., Rothia mucilaginosa, and Pantoea aggl merans were identified (Table 3) (Fig 4).
Table 3: Identified bacteria by Microscan devices based on the morphological, biochemical, and drug-resistance pattern using an automated Microscan device.
| Sample No. | Result |
| 11-O** (2) | Staphylococcus aureus |
| 11-O | Staphylococcus aureus |
| 3-M* | Staphylococcus aureus |
| 8-M | Staphylococcus schleiferi |
| 6-O | Staphylococcus epidermidis |
| 11-M | Micrococcus sp. |
| 2-M | Micrococcus sp. |
| 12-M | Rothia mucilaginosa |
| 3-O | Pantoea agglomerans |
*(M) Microbiology students; ** (O) Other students
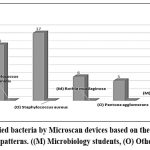 |
Figure 4: Identified bacteria by Microscan devices based on the morphological, biochemical, patterns. ((M) Microbiology students, (O) Other students). |
Antibiotic susceptibility of the bacterial strains
Antibiotic sensitivity of S. aureus strains isolated from mobile phones. The isolated S. aureus was Ampicillin and polymyxin B resistant. It was intermediate against the tested sulfamethoxazole and Bacitracin. S. aureus isolated from microbiology students, and non-microbiology students showed no variation in antibiotic sensitivity patterns. All Staphylococcus aureus strains were vancomycin and gentamicin-sensitive (Table 4). The S. epidermidis isolate showed resistance against Polymyxin B and exhibited an intermediate response against sulfamethoxazole and bacitracin (Table 5). The isolated Micrococcus sp. exhibited resistance against polymyxin B, whereas it showed an intermediate response against sulfamethoxazole and was sensitive against other tested antibiotics (Table 6). The isolated strains, Rothia mucilaginosa-12-M, and Pantoea agglomerans-3-O were sensitive against the tested antibiotics. Bacillus sp. isolated from the mobile phones of the microbiology students exhibited sensitivity except for Erythromycin (Table 7).
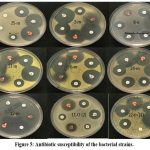 |
Figure 5: Antibiotic susceptibility of the bacterial strains. |
Table 4: Analysis of drug resistance pattern of opportunistic S. aureus strains isolated from the surface of the mobile phone.
| Samples | Antimicrobial Agent | Antibioticsµg or U | Zone of inhibition diameter (mm) | Susceptibility |
| S. aureus -11-O* (2) | Ampicillin (AMP) | 10 µg | 15 | R |
| Sulfamethoxazole | 50 µg | 20 | I | |
| Bacitracin (BA) | 8 U | 20 | I | |
| Vancomycin (VA) | 30 µg | 18 | S | |
| Polymyxin B (PB) | 300 U | 11 | R | |
| Gentamicin (GM) | 10 µg | 25 | S | |
| S. aureus -11-O* | Ampicillin (AMP) | 10 µg | 15 | R |
| Gentamicin (GM) | 10 µg | 20 | S | |
| Vancomycin (VA) | 30 µg | 19 | S | |
| S. aureus -3-M** | Ampicillin (AMP) | 10 µg | 14 | R |
| Vancomycin (VA) | 10 µg | 23 | S | |
| Gentamicin (GM) | 30 µg | 25 | S |
*Non-microbiology students; ** Microbiology students; R – resistant; S – sensitive
Table 5: Analysis of drug resistance pattern of opportunistic S. epidermidis and S. schleiferi strains isolated from the surface of the mobile phone.
| Samples | Antimicrobial Agent | Antibiotics(µg or U) | Zone of inhibition diameter (mm) | Susceptibility |
| S. epidermidis-6-O | Ampicillin (AMP) | 10 µg | 20 | R |
| Sulfamethoxazole | 50 µg | 15 | I | |
| Bacitracin (BA) | 8 U | 18 | I | |
| Vancomycin (VA) | 30 µg | 20 | S | |
| Polymyxin B (PB) | 300 U | 18 | R | |
| Gentamicin (GM) | 10 µg | 33 | S | |
|
S. schleiferi– 8-M |
Ampicillin (AMP) | 10 µg | 30 | S |
| Vancomycin (VA) | 30 µg | 29 | S | |
| Gentamicin (GM) | 10 µg | 31 | S |
I – Intermediate; R – Resistant; S – Sensitive.
Table 6: Analysis of antibiotic susceptibility pattern of opportunistic Micrococcus strains isolated from the surface of the mobile phone.
| Samples | Antimicrobial Agent | Antibioticsµg or U | Zone of inhibition diameter (mm) | Susceptibility |
| Micrococcus sp.-2-M | Ampicillin (AMP) | 10 µg | 33 | S |
| Sulfamethoxazole | 50 µg | 20 | I | |
| Bacitracin (BA) | 8 U | 33 | S | |
| Vancomycin (VA) | 30 µg | 27 | S | |
| Polymyxin B (PB) | 300 U | 18 | R | |
| Gentamicin (GM) | 10 µg | 30 | S | |
| Micrococcus sp.-11-M | Ampicillin (AMP) | 10 µg | 28 | S |
| Sulfamethoxazole | 50 µg | 20 | I | |
| Bacitracin (BA) | 8 U | 30 | S | |
| Vancomycin (VA) | 30 µg | 25 | S | |
| Polymyxin B (PB) | 300 U | 16 | R | |
| Gentamicin (GM) | 10 µg | 30 | S |
I – Intermediate; R – Resistant; S – Sensitive
Table 7: Analysis of antibiotic susceptibility pattern of Bacillus sp. isolated from the surface of the mobile phone.
| Samples | Antimicrobial Agent | Antibiotics(µg or U) | Zone of inhibition diameter (mm) | Susceptibility |
| Bacillus simplex-24-M | Vancomycin (VA) | 30 µg | 23 | S |
| Trimethoprim | 2.5 µg | 35 | S | |
| Tetracycline (TE) | 10 µg | 25 | S | |
| Clindamycin (DA) | 2 µg | 23 | S | |
| Erythromycin (E) | 15 µg | 20 | I | |
| Gentamicin (GM) | 10 µg | 32 | S | |
| Bacillus clausii-25-M | Vancomycin (VA) | 30 µg | 24 | S |
| Trimethoprim | 2.5 µg | 32 | S | |
| Tetracycline (TE) | 10 µg | 11 | R | |
| Clindamycin (DA) | 2 µg | >25 | S | |
| Erythromycin (E) | 15 µg | >25 | S | |
| Gentamicin (GM) | 10 µg | 33 | S | |
| Bacillus megaterium-22-M | Vancomycin (VA) | 30 µg | 21 | S |
| Trimethoprim | 2.5 µg | 26 | S | |
| Tetracycline (TE) | 10 µg | 23 | S | |
| Clindamycin (DA) | 2 µg | >25 | S | |
| Erythromycin (E) | 15 µg | 32 | S | |
| Gentamicin (GM) | 10 µg | 30 | S |
I – Intermediate; R – Resistant; S – Sensitive
β-lactamase producing Staphylococcus strains
β–lactamase producing Staphylococcus strains were isolated from the students associated with microbiology and other subjects. Antibiotic susceptibility analysis between coagulase-positive and coagulase-negative Staphylococcus was depicted in Table 8. β–lactamase producing Staphylococcus strain was sensitive to Gentamicin and Vancomycin, whereas resistant to Ampicillin.
Table 8: Antibiotics susceptibility analysis between coagulase-positive and coagulase-negative Staphylococcus.
| Categories | Antibiotic | Disk content | Microbiology students | Other students | |
| Coagulase positiveStaphylococcus | S. aureus (O-11) | Gentamicin | 10 µg | – | S |
| Ampicillin | 10 µg | – | R-BLAC* | ||
| Vancomycin | 30 µg | – | S | ||
| S. aureus (M-3) | Gentamicin | 10 µg | S | – | |
| Ampicillin | 10 µg | R (BLAC*) | – | ||
| Vancomycin | 30 µg | S | – | ||
| Coagulase negativeStaphylococcus | S. epidermidis (O-6) | Gentamicin | 10 µg | – | S |
| Ampicillin | 10 µg | – | S | ||
| Vancomycin | 30 µg | – | S | ||
| S. schleiferi (M-8) | Gentamicin | 10 µg | S | – | |
| Ampicillin | 10 µg | S | – | ||
| Vancomycin | 30 µg | S | – | ||
* (BLAC) = Beta-lactamase positive.
Discussion
This study investigated bacterial contamination on microbiology and other students’ mobile phones at King Saud University. Tagoe and colleagues (2011) found microbial contamination on 100 phones due to poor hygiene.24 We found bacteria on 56 (93%) phones, including 27 (90%) from microbiology students and 29 (96%) from others. Many students in both groups used their phones in the toilet, indicating inadequate cleaning.
Our results showed significant differences among microbiology students: 23 (77%) used phones in toilets, 7 (23%) didn’t, and others (non-microbiology students) 21 (70%) did. Matthew Olsen and colleagues (2021) found that 52% of participants (n=86) used their devices in the bathroom, emphasizing the unhygienic environments where mobile devices and smartphones are constantly utilized.25
Only 9 (30%) microbiology students cleaned their phones regularly with disinfectant, while 21 (70%) didn’t. Among non-microbiology students, 7 (23%) used disinfectant, and 23 (77%) didn’t. In the microbiology lab, 90% (n = 27) of microbiology students followed standard operating procedures and didn’t use mobile phones; only 3 did. Zakai and others showed significant differences in disinfectant use between microbiology students 9 (30%) and others 21 (70%), similar to non-microbiology students 7 (23%) who used the disinfectant too, while 23 (77%) did not use it.16
All these previous results revealed inadequate cleaning of mobile phones. In the present study, 56 (93%) mobile phones were contaminated with bacteria, 27 (90%) were obtained from microbiology students, and 29 (96%) were obtained from other students. In contrast, another study in Nigeria was reported by Amala, S. and I. Ejikema, who Found that contamination rates (80.6%),26 and another study conducted by Algmati, A. A. M, found that the prevalence of organisms in students’ mobile phones was (60.8%).27
Several studies have demonstrated that the most common Gram-positive bacterium isolated from mobile phone surfaces is Staphylococcus.28 Our finding also identified Staphylococcus as the major strain which is a greater concern due to its virulence. Staphylococci were the most represented bacteria, making mobile phones susceptible to contamination due to normal skin saprophytes.29 Staphylococcus aureus, Staphylococcus schleiferi, and Staphylococcus epidermidis were determined. Other bacterial species identified included Micrococcus sp., Rothia mucilaginosa, and Pantoea aggl merans. β-lactamase producing Staphylococcus strains were isolated from both microbiology and other students, in this study. Panganai, T. and P. Hamadziripi study showed that seventeen (68%) of mobile devices were contaminated with E coli, (75%), Staphylococci (38%), and Streptococcal (21%) which are pathogens that have a potential of causing nosocomial infections.4
The isolated bacteria in this study showed resistance against certain antibiotics but not against Vancomycin and Gentamycin. Recent studies have determined the prevalence of microbial contamination of mobile cell phones among human populations and individuals.30-33 Also, according to Sadeeq’s study. both the automated system and disc diffusion technique, antibiotic susceptibility patterns performed for P. aeruginosa, Pseudomonas stutrezi (P. stutrezi), Aeromonas spp., Acinetobacter baumanni (A. baumanni) that collected from the surfaces of mobile phones showed that all isolates were susceptible to all tested antibiotics.34, 35
Conclusions
Mobile phones of both microbiology students and others of King Saud University were found to be contaminated with bacteria. The pervasiveness of pathogenic bacteria from the mobile phones of microbiology students has been determined, and the result was compared with other students. The determined bacterial strains were more resistant to ampicillin than other tested antibiotics. The absence of cleaning behavior for mobile phones is a major factor in transmitting bacteria from the mobile phone to others or different environments. Moreover, disinfectants could reduce the microbial load on the mobile phone surface. Students should clean their hands with disinfectants before handling the mobile phone. It is important to implement standard guidelines for using mobile phones. Further studies are required to analyze the drug-resistant gene, and mechanism of action, including β-lactamase production. Finally, more studies are needed to determine the survival time of pathogens on cell phones.
Acknowledgment
The authors thank King Saud University, Riyadh, Saudi Arabia, for supporting this work.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Author Contributions
Conceptualization: Roua Mohammad Saleh ALkufeidy; Mohamed Abdellatif El-Tayeb and Shuruq Ahmed Othman Alshabanat.
Writing, original draft preparation:Roua Mohammad Saleh ALkufeidy., and Mohamed Abdellatif El-Tayeb.
Writing, review and editing: Mohamed Abdellatif El-Tayeb.
Visualization: Mshael Mohammed Thabit Bin Madhi. Supervision, Roua Mohammad Saleh ALkufeidy, and Mohamed Abdellatif El-Tayeb
Data curation: Noura Saleem Duhaim Aldosari. and Nura Suliman Abdullah Alsakabi.
All authors have read and agreed to the published version of the manuscript.
References
- Tajouri L, Campos M, Olsen M, Lohning A, Jones P, Moloney S, et al. The role of mobile phones as a possible pathway for pathogen movement, a cross-sectional microbial analysis. Travel Med Infect Dis 2021; 43:102095.
CrossRef - Dhayhi N, Kameli N, Salawi M, Shajri A, Basode VK, Algaissi A, Alamer E, Darraj M, Shrwani K, Alhazmi AH. Bacterial Contamination of Mobile Phones Used by Healthcare Workers in Critical Care Units: A Cross-Sectional Study from Saudi Arabia. Microorganisms. 2023; 11(8):1986.
CrossRef - Hikmah N. A, and Anuar T.S. Mobile phones: a possible vehicle of bacterial transmission in a higher learning institution in Malaysia. MJMS, 2020. 27(2): p. 151.
CrossRef - Panganai T. and P. Hamadziripi. Health worker’s mobile phone: Could it be a danger to patients’ health or an innovation for health? Internat J of Scie and Resear Arch, 2023. 10 (1): p. 695-702.
CrossRef - Robinson T, Cronin T, Ibrahim H, et al. Smartphone use and acceptability among clinical medical students: a questionnaire-based study. J Med Syst. 2013;37(3):9936. doi:10.1007/s10916-013-9936-5.
CrossRef - Hamidu M. R. and Yunusa S. H., Isolation and Identification of Microorganisms from Mobile Phones of staff and students of Yusuf Maitama Sule University, Kano. BIMA J of Scie and Techno. 2024. 8(2A): p. 287-292.
- Olaitan O. L, David A. O, Michael O. A. Deep Learning Approach for Classification of Tweets in Detecting Cyber Truculent. Adv. Res. 2024. 25(2): p. 113-122.
CrossRef - Behrouzmanesh F., et al., Prevalence and genetic characteristics of Staphylococcus aureus isolates from cell phones of medical students from Iran. Acta Microbiologica et Immunologica Hungarica, 2024.
CrossRef - Hamdan-Partida A, González-García S, Martínez-Ruíz FJ, Zavala-Sánchez MÁ, Bustos-Hamdan A, Bustos-Martínez J. Molecular Characterization of Staphylococcus aureus Strains Isolated from Mobile Phones. Microorganisms. 2022; 10(3):669.
CrossRef - Tekerekoǧlu MS, Duman Y, Serindağ A, et al. Do mobile phones of patients, companions and visitors carry multidrug-resistant hospital pathogens?. Am J Infect Control. 2011;39(5):379-381.
CrossRef - Kapdi M, Hoskote SS, Joshi SR. Health hazards of mobile phones: an Indian perspective. J Assoc Physicians India. 2008; 56:893-897.
- Selim H. S, Abaza A. F. Microbial contamination of mobile phones in a health care setting in Alexandria, Egypt. GMS Hyg Infect Control. 2015;10: Doc 03.
- Saxena S, Singh T, Agarwal H, Mehta G, Dutta R. Bacterial colonization of rings and cell phones carried by health-care providers: are these mobile bacterial zoos in the hospital?. Trop Doct. 2011;41(2):116-118.
CrossRef - Chawla K, Mukhopadhayay C, Gurung B, Bhate P, Bairy I. Bacterial ‘Cell’ Phones: Do cell phones carry potential pathogens? Online J Health Allied Scs. 2009;8(1):8
- Nwankwo E. O, Ekwunife N, Mofolorunsho K. C. Nosocomial pathogens associated with the mobile phones of healthcare workers in a hospital in Anyigba, Kogi state, Nigeria. J Epidemiol Glob Health. 2014;4(2):135-140.
CrossRef - Zakai S, Mashat A, Abumohssin A, et al. Bacterial contamination of cell phones of medical students at King Abdulaziz University, Jeddah, Saudi Arabia. J Microsc Ultrastruct. 2016;4(3):143-146.
CrossRef - Almakishah N. H. Accumulation of Microbial Contamination on Keyboards and Mobile Phone Devices in the University Community. Egyp J of Microbiol, 2024. 59(1): p. 15-27.
CrossRef - Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis [published correction appears in Lancet. 2022 Oct 1;400(10358):1102.
- Olsen M, Nassar R, Senok A, et al. Mobile phones are hazardous microbial platforms warranting robust public health and biosecurity protocols. Sci Rep. 2022;12(1):10009.
CrossRef - Ngema Y, Ndou S, Pietrzak J, Sikhauli K. Microbial Contamination of Cellphones of Healthcare Workers in The Orthopaedic Department at a Tertiary Institute In Gauteng. Orthop Procs. 2023;105-B(SUPP_15):32-32.
CrossRef - William G. Walter “Standard Methods for The Examination of Water and Wastewater (11th ed.)”, Ameri J of Public Health 51, no. 6 (June 1, 1961): pp. 940-940.22.
CrossRef - McGregor A, Schio F, Beaton S, Boulton V, Perman M, Gilbert G. The MicroScan WalkAway diagnostic microbiology system–an evaluation. Pathology. 1995;27(2):172-176.
CrossRef - Al Farraj D. A., et al., Enhanced production, purification and biochemical characterization of therapeutic potential fibrinolytic enzyme from a new Bacillus flexus from marine environment. J of King Saud University-Science, 2020. 32(7): p. 3174-3180.
CrossRef - Clinical and Laboratory Standard Institute (CLSI) (2020) Performance Standards for Anti-Microbial Susceptibility Testing. 30th Edition, M100.
- Tagoe D. N, Gyande V. K, Ansah E. O. Bacterial Contamination of Mobile Phones: When Your Mobile Phone Could Transmit More Than Just a Call. Web med Central Microbiology. 2011;2(10):1-9.
- Olsen M, Lohning A, Campos M, et al. Mobile phones of paediatric hospital staff are never cleaned and commonly used in toilets with implications for healthcare nosocomial diseases. Sci Rep. 2021;11(1):12999.
CrossRef - Amala S. and Ejikema I. Bacteria Associated with the Mobile Phones of Medical Personnel. American Journal of Biomedical Sciences, 2015. 7(1).
CrossRef - Algmati A.A.M., et al., Prevalence and Risks of Mobile Phone Microbial Contamination Among Medical, Dental, and Health Sciences Students in The Healthcare Setting. 2024.
- Yao N, Yang XF, Zhu B, et al. Bacterial Colonization on Healthcare Workers’ Mobile Phones and Hands in Municipal Hospitals of Chongqing, China: Cross-contamination and Associated Factors. J Epidemiol Glob Health. 2022;12(4):390-399.
CrossRef - Maurici M, Pica F, D’Alò GL, et al. Bacterial Contamination of Healthcare Students’ Mobile Phones: Impact of Specific Absorption Rate (SAR), Users’ Demographics and Device Characteristics on Bacterial Load. Life (Basel). 2023;13(6):1349.
CrossRef - Al-Abdalall AH. Isolation and identification of microbes associated with mobile phones in Dammam in eastern Saudi Arabia. J Family Community Med. 2010;17(1):11-14.
CrossRef - Elmanama A, Hassona I, Marouf A, Alshaer G, Abu Ghanima E. Microbial load of touch screen mobile phones used by university students and healthcare staff. Journal of the Arab Ameri Univers, 2015. 1(1): p. 1-18.
CrossRef - Al-Abdalall AH. Isolation and identification of microbes associated with mobile phones in Dammam in eastern Saudi Arabia. J Family Community Med. 2010;17(1):11-14.
CrossRef - Chauhan A, Garg S, Ranjan AA, et al. Prevalence of microbial contamination of mobile cell phones in general population of Delhi, India. J Exp Clin Microbiol 2018;1(1):12-15.
- Sadeeq T, Arikan A, Sanlidag T, Guler E, Suer K. Big Concern for Public Health: Microbial Contamination of Mobile Phones. J Infect Dev Ctries. 2021;15(6):798-804.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



