

How to Cite | Publication History | PlumX Article Matrix
Sadegh Hasannia, Shirin Jalili and Reyhaneh Sariri*
Department of Biology, The University of Guilan, Rasht Iran.
ABSTRACT: Cholesteryl ester transfer protein (CETP) catalysis the exchange of triglycerides (TG) and cholesterol esters among plasma lipoproteins. It has been shown that variations at CETP locus is important in the levels and activity of CETP and high density lipoprotein (HDL) plasma concentration. In this research, we assessed the relationship between TaqIB CETP polymorphism and high density lipoprotein-cholestrol (HDL-C) concentration in a study sample of 128 Iranian residents. 1Based on our investigations, it was shown that presence of B1B1 genotype related to TaqIB polymorphism was negatively correlated with HDL-C and HDL2-C, but positively correlated with LDL-C. On the other hand, no correlation with HDL3-C was observed. Analysis of HDL-C subfraction in CHD and control subjects revealed that variation of the CETP TaqI B locus was significantly associated with concentration of HDL2-C subclass. Homozygous and heterozygous carried the B2 alleles, compared with B1 homozygote had significantly elevated concentration of cholesterol distribution in HDL. We concluded that variation at the CETP gene locus is a significant determinant of HDL-C levels and CETP activity. Moreover, these effects appear to translate into a lower CHD risk among patients with B2 allele.
KEYWORDS: Cholesteryl ester transfer protein; Gene Polymorphisms; HDL-C; Taq1B; RFLP
Download this article as:| Copy the following to cite this article: Hasannia S, Jalili S, Sariri R. The Relationship Between Cholestryl Ester Transfer Protein Taq I Genotype and Plasma Level of HDL Subgroups in Coronary Heart Disease. Biosci Biotechnol Res Asia 2008;5(1) |
| Copy the following to cite this URL: Hasannia S, Jalili S, Sariri R. The Relationship Between Cholestryl Ester Transfer Protein Taq I Genotype and Plasma Level of HDL Subgroups in Coronary Heart Disease. Biosci Biotechnol Res Asia 2008;5(1) Available from: https://www.biotech-asia.org/?p=6998 |
Introduction
CETP catalysis the exchange of triglycerides (TG) and cholesterol esters among plasma lipoproteins, a key step in reverse cholestrol transport (RCT) in humans. Although the antiatherogenic properties of HDL have not been fully elicidated, it has been suggested that HDL exerts its cardioprotective function through RCT [1]. RCT is a metabolic pathway initiated by HDL-mediated efflux from peripheral tissues and subsequent delivery to the liver [2]. In human, CETP mRNA encodes a polypeptide of Mr 53000, which is N-glycosylated at 4 sites, giving rise to the mature from of CETP of Mr 74000 [1]. CETP is a hydrophilic glycoprotein that is secreted mainly from the liver and that circulate in plasma, bound to HDL. Some lower levels of the protein is also secreted from spleen, and adiopse tissues, and lower levels have been detected in the small intestine, adrenal gland, heart, kidney, and skeletal muscle [2]. The CETP gene encompasses 16 exons, and it is located on chromosome 16q21 adjacent to the lecithin-cholestrol acyltransferase gene. CETP net transfer of cholesterol from HDL to very low density lipoprotein (VLDL), low density lipoprotein (LDL) and chylomicron in exchange for triglycerides (TG) [3]. The importance of CETP activity in the metabolism and composition of HDL particles is clearly demonstrated in individuals with genetic CETP deficiency [4-6]. The restriction site, TaqI B polymorphism of CETP, is an important regulatory factor of lipid metabolism especially in plasma HDL-C and LDL-C levels in patient with CHD [7, 8]. HDL-C levels have been shown to be intensively and independently correlated with the risk of CHD. It has been shown that high HDL-C equal to or greater than 60 mg/dL as a negative risk factor for CHD.
In this study, we assessed the relationship between TaqIB CETP polymorphism and high density lipoprotein-cholestrol (HDL-C) concentration in a study sample of 128 patients with CHD from Heshmat heart hospital in Rasht.
Materials and Methods
Subjects
The study population consisted of 142 patients selected based on the result of their angiography from heart center of Heshmat hospital in Rasht. A total of 14 patients were excluded from the study due to having one or more of the following factors:
Diabetes melitus (fast blood sugar FBS>140 mg/dL)
History of using insulin or oral antibiotics
Miocardic heart attack within the last 6 weeks
The use of lipid lowering drugs
History of cronary surgery
History of major sugeries within the last 6 weeks
History of surgery, lack of activities and being in hospital during the last 4 weeks.
After these exclusions, 128 subjects remained eligible for this study. Informations on smoking, eating habits and exercise were obtained by interview.
Plasma lipid and lipoproteins
Blood samples were obtained by venipuncture into vacum tubes containing EDTA after an overnight (14 hours) fast. Plasma was immediately centrifuged at 2000 rpm for 15 minutes and the samples were delivered immediately (4°C) to our laboratory and stored at -20°C until use for lipid measurement and genotyping. Plasma total cholestrol (TC) and TG levels were measured by enzymatic methods, while the lipoprotein subgroups were measured using polyanion precipitation method.
Determination of total cholestrol (TC)
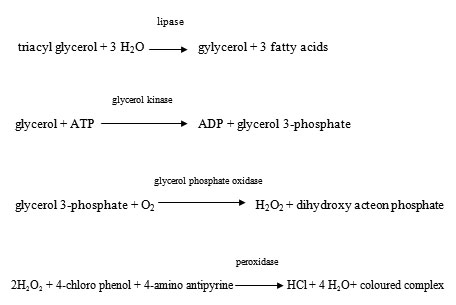
In this enzymatic method, total plasma cholestrol was converted to free cholestrol by the action of cholestrol esterase. The free cholestrol was then oxidized to cholest-4-ox-3-one and the librated H2O2 produced a coloured complex from phenolic substrate in the presence of peroxidase. The intensity of the colour was related to the total plasma cholestrol which was measured at 570 nm using a known cholestrol solution as standard.
Determination of plasma triglyceide ( TG)
The following enzymatic reaction were the basis of the procedure used for determination of plasma triacyl glycerols. The intensity of the coloured complex was measured spectrophotomerically at 500 nm in the presence of a standard triglyceride solution.
Isolation of HDL from other lipoproteins
100 ml DS-MgCl2 (dextran sulphate 10g/lit and MgCl2 500mmol/lit) was added to 1 ml plasma. The test tube was left at room tempreature for 10 minutes after mixing for 3 seconds. The tube was kept at 4°C for 30 minutes,centrifuged at 1500 rpm and the concentration of cholestrol was then measured in the supernatant. Another portion of the supernatant was used for separation of HDL subunits.
Measurement of HDL2 and HDL3
50 ml of SD-MgCl2 solution was added to 0.5 ml of the supernatant and the mixed for 3 seconds. The tube was centrifuged at 4°C after remaining at room temperature for 10 minutes. The supernatant contaning HDL3 was used for appropriate measurement. The quantity of HDL2 was then obtained by substracting this amount from HDL-C.
TaqIB polymorphism of CETP gene
Genomic DNA was extracted from blood leukocytes by a simple salting out method described by Müller [9]. A fragment of 535 bp in intron 1 of the CETP gene was amplified with polymerase chain reaction (PCR) in a DNA Thermal Cycler (PTC-100, MJ Research, Inc) using ologonucleotide primers (forward 5′-CACTAGCCCAGAGAGAGGAGTGCC-3′, reverse 5′-CTGAGCCCAGCCGCACACTAAC-3′. Each amplification was performed by using 2 ml of DNA template in a volume of 25 ml containing 1 ml of each primer, 0.5 ml of dNTP, 1.1 ml MgCl2, 0.5 ml Taq polymerase and 16.5 ml deionized water. DNA templates were denatured at 95°C for 10 minutes, and then each PCR was subjected to to 30 cycles with a temperature cycle consisting of 95°C for 3 minutes, 62 °C for 35 seconds, 72°C for 45 seconds, and finally, an extension at 72°C for 10 minutes. The PCR products were subjected to restriction enzyme analysis by digestion with 1.5 ml of the restriction endonuclease TaqI for 10 ml of PCR sample at 65°C for 16 hours in the buffere ecommended by the manufacturer, and the fragments were separated by electrophoresis on an 1.5% agarose gel. Gel-duct instrument was used for visualization of DNA fragments at the end of electrophoresis run. The resulting fragments were 174 and 361 bp for the B1 allele and 535 bp for the uncut B2 allele.
Statistical analyses
Statistical analysis was carried out using one of the most common and reliable softwares i.e. statistical anaylsis system (SAS) software. A sensitivity analysis was carried out to estimate the validity and precision of the regression coefficients for the CETP genotype variables when additional independent terms were included into the model.
Results and discussions
Subject charateristics
We analyzed a total of 142 subjects, 43 controls and 85 patients who were registered in Heshmat heart hospital of Rasht and diagnosed with CHD according to the results of their angiography. The frequency and phenotype association of the TaqIB-CETP polymorphism was investigated at the population level. Table 1 represents a summry of the biochemical characteristics of the participants. The mean age of both control and CHD group was 51.5 and 51.6 respectively, all subjects were male and non-smokers.
It is evident from the data in Table 1 that there is a noticeable difference in HDL2, HDL-C, LDL, TG and TC values between the two groups (CHD and control). On the other hand, the values of HDL3-C show negligible differences with a p-value of 0.95 compared to 0.0001 in other cases.
The effrect of TaqIB polymorphism with plasma lipids and liporoteins
The relationship between genotyping and biochemical characteristics in control and CHD groups was investigated using Logestic regression analysis with the GLM procedure and SAS software and the resluts are presented in Table 2. The results presented in Table 2 demonstrate that homozygotes for the B1 allele had lower HDL-C than levels did B1B2 and B2B2. It has been shown that a similar association exists for apo-A values and that the results are similar between male and female subjects in a similar age grouping [8].
Conclusions
According to the results obtained from this study, the foolowing conclusion remarks could be made:
Presence of B1B1 genotype related to TaqIB polymorphism was negatively correlated with HDL-C and HDL2-C, and positively correlated with LDL-C.
There was no correlation between B1B1 genotype and HDL3-C. Analysis of HDL-C subfraction in CHD and control subjects revealed that variation of the CETP TaqI B locus was significantly associated with concentration of HDL2-C subclass.
Homozygous and heterozygous carried the B2 alleles, compared with B1 homozygote had significantly elevated concentration of cholesterol distribution in HDL.
Variation at the CETP gene locus is a significant determinant of HDL-C levels and CETP activity.
Moreover, these effects appear to translate into a lower CHD risk among patients with B2
References
- Ikewaki K., Mabuchi H., Teramato T., et al. association of cholestryl ester transfer protein activity and TaqIB polymorphism with lipoprotein variation in Japanese subjects. Metabolism. 52(12), 1564-70 (2003).
- Expert panel on detection, evaluation and treatment of high blood cholestrol in adults; Excutive summary of the Third Report of the National Cholestrol Education Program (NECP). JAMA.285, 2486-97 (2001).
- Tall A.R. Plasma cholestryl ester transfer protein and high density lipoproteins: New insights from molecular genetics studies. J. Intern. Med. 237, 5-12 (1995).
- Yamashita S., Matsuzawa Ym Okazaki M., et al. Small polydisperse low density lipoproteins in familial hyperalphalilipoproteinemia with complete deficiency of cholestryl ester transfer activity. Atherosclerosis. 70, 7-12 (1988).
- Ikewaki K., Rader D.J., Sakamoto T., et al. Delayed catabolism of high density lipoprotein apolipoproteinA-I and A-II in human cholestry ester transfer protein deficiency. J. Clin. invest. 92, 1650-58 (1993).
- Ikewaki K., Nishiwaki M., Sakamoto T., et al. Increased catabolic rate of low density lipoproteins in human with cholestryl ester transfer protein deficiency. J. Clin. Invest. 96, 1573-81 (1995).
- Kuivenhoven J.A., Jukema J.W., Zwinderman A.H., et al. The role of a common variant of the cholestryl ester transfer protein gene in the progression of coronary atherosclerosis. The regression Growth Evaluation Statin Study Group. New Eng. J. Med. 338, 86-93 (1998).
- Ordovas J.M., Cupples L.A., Corella D., et al. Association of cholestryl ester transfer protein-TaqIB polymorphism with variations in lipoprotein subclasses and coronary heart disease risk. The Farmingham Study. Arterioscler Thromb Vase Biol. 20, 1323-29 (2000).
- Müller S.A,. Dykes D.D., Polesky H.F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acid Res. 16, 1215-19 (1989).

This work is licensed under a Creative Commons Attribution 4.0 International License.



