

Manuscript accepted on : May 29, 2011
Published online on: 28-06-2011
Whether Paternal Age Effect Exists as a Risk Factor in Trisomy 21
Minakshi Vashist1, Neelkamal2* and Amit Kumar3
Department of Genetics, Maharshi Dayanand University, Rohtak, Haryana India.
ABSTRACT: Background Down syndrome (Trisomy -21) is a most common aneuploid condition caused by the presence of an extra 21 chromosome and is a major cause of mental retardation. The only etiological factor that has been established in literature is advanced maternal age for the occurrence of trisomy 21 but little is known about the genetic consequences of advanced paternal age. The study was carried out to find the effect of paternal age on trisomy-21. Methodology Present study has been conducted on 200 cases of Down syndrome from 30 centers of 12 districts of Haryana. These patients were subjected to detailed morphogenetic & cytogenetic analysis. Results & conclusion Variability in age of father was found at the birth of mongoloid child. It varied from 19 years to the 48 years. Most of the Down syndrome cases (63) were born from the father of age between 31-35 years. Correlation between father’s age and number of Down syndrome cases (keeping mother age constant) came out as r = 0.041. Partial correlation coefficient showed that increase risk of Down syndrome may be due to combined effect of advanced parental age. Down syndrome cases born to father of less than 30 years of age were 40.5% while those born to more than 30 years of age were 59.5%. The existence of a paternal age effect on Down syndrome is controversial but an important factor & it should not be ignored in morphological & cytogenetic analysis of patients.
KEYWORDS: Down syndrome; human genetics; nondisjunction; Paternal age; Trisomy 21
Download this article as:| Copy the following to cite this article: Vashist M, Neelkamal, Kumar A. Whether Paternal Age Effect Exists as a Risk Factor in Trisomy 21. Biosci Biotech Res Asia 2011;8(1) |
| Copy the following to cite this URL: Vashist M, Neelkamal, Kumar A. Whether Paternal Age Effect Exists as a Risk Factor in Trisomy 21. Biosci Biotech Res Asia 2011;8(1). Available from: https://www.biotech-asia.org/?p=9337 |
Introduction
Down syndrome is a model for study of human aneuploidy and is usually associated with the presence of extra chromosome 21 and is characterized by a complex phenotype including characteristic facial features, skeletal appearance and low mental level.The disease was first described in man by John Langdon Down (1866)1 and was originally called mongolian idiocy or mongolism. It is a cosmopolitan disease, having been reported in nearly all countries and ethnic groups.The incidence of Down syndrome is of the same magnitude all over the world i.e. 1 in 700 overall births (Kotzot and Schinzel 2000)2. The natural history of Down syndrome in childhood is characterized mainly by developmental delay, growth retardation, and
immunodeficiency. Individuals with Down syndrome have more behavioral and psychiatric problems than other children but fewer than other individuals with mental retardation. About 90-95% of Down syndrome cases are due to free trisomy 21. Another 2-4% has chromosomal rearrangement such as translocation with acrocentric chromosome resulting in trisomy 21. The remaining 2-4% of Down syndrome patients shows mosaicism for trisomy 21 and normal cell line. (Pangalos et al. 1994;3 Vashist et al. 2009;4 Kaur A and Singh J.R 20105). Known reason for the conceptions of trisomies is delayed fertilization, advanced maternal age and increased satellite associations (Fox and Sindwani 19856; Ghalib and Issac 19917). However some lifestyle factors such as smoking, alcohol drinking and caffeine consumption have been investigated and no consistent association between disomy frequency and any type of lifestyle factors has been established (Shi and Martin 20008).
Increase in parental age has become a public health concern because more infants are being born who are at high risk for genetic disorders & identification of potential risks associated with advanced parental age is now more relevant than ever. The influence of maternal age in Down syndrome is well established but little is known about the genetic consequences of advance paternal age and has not been clearly defined. The question whether there is a paternal age effect on male nondisjuction remains uncertain. The existence of a pater nal age effect on Down syndrome is controversial. There are several possible explanations for the failure to conclusively identifying these factors. It may be that the concerned factors have not been studied yet. In this paper we attempted to define whether a paternal age effect exists as a risk factor in Down syndrome.
Material and Methods
Present study has been conducted on 200 cases of Down syndrome from 30 centers of 12 districts of Haryana. There were 152 male & 48 female patients. These patients were subjected to detailed morphogenetic, cytogenetic analysis after the written consent of the father /guardian.
Morphogenetic Analysis
A questionnaire has been developed to record all the required information about family history including age of the parents at the birth of the child.
Cytogenetic Analysis
For cytogenetic analysis the peripheral blood samples of Down syndrome patients and normal persons were taken with the help of clinician after the consent of the parent/guardian. The blood sample was subjected to culture in a nutritional media. Peripheral blood samples of Down syndrome patients (with the help of qualified technician) were collected in heparanised vacutainer tube and subjected to culture in the laboratory using media RPMI-1640, supplemented with phytohaemagglutinin, antibiotics and foetal calf serum. Blood culture was set up at 37oC for 72 hours.The cultured cells were treated with colchicine forty five minutes prior to harvesting.
Result
Mean paternal age of Down syndrome cases at the time of conception was recorded 31.5 years. Variability in age of father was found at the birth of mongoloid child. It varied from 19 years to the 48 years. Most of the Down syndrome cases
were born from the father of age between 31-35 years (Table1 & Figure1). Correlation between father’s age and number of Down syndrome cases (keeping mother age constant) came out as r =0.041 (Table 1). Slightly positive value of Partial correlation coefficient showed that increase risk of Down syndrome may be relates to paternal age. Down syndrome cases born to father of less than 30 years of age (<30) were 40.5% while those born to more than 30 years of age. (>30) were 59.5% (Table 2 and Figure 2).
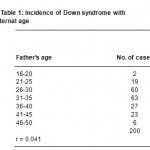 |
Table 1: Incidence of Down syndrome with paternal age.
|
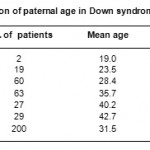 |
Table 2: Distribution of paternal age in Down syndrome cases (n=220).
|
Age and sexwise analysis of Down syndrome cases in different age group of parents showed that more number of male Down syndrome children was born to parents of 25 to 30 years of age. There were 22.5% males and 7.5% females born from father’s age between 25-30 years (Table 3).
Table 3: Age and sexwise distribution of Down syndrome cases in different paternal age groups during pregnancy
|
Age of parents (in years) |
<20 |
21-25 |
25-30 |
31-35 |
36-40 |
41-45 |
>45 |
| ** | ** | ** | ** | ** | ** | ** | |
|
Male child (%) |
1 |
7.5 |
22.5 |
22 |
11 |
11 |
1 |
| Female child (%) | – | 2 | 7.5 | 9.5 | 2.5 | 2 | 0.5 |
| Total (%) | 1 | 9.5 | 30 | 31.5 | 13.5 | 13 | 1.5 |
In free trisomy 21 Down syndrome cases, father’s age at birth of Down syndrome child was between 20-46 years and in mosaic cases it was 35 and 37 years (Table 4). Father’s age was above 30 in 76.7% of cytogenetically analysed Down syndrome cases and below 30 in 32.3% of cases (Table 5). In free trisomy 21, father’s age was below 30 in 24.7% cases and above 30 in 75.2% of cases
(Table 6).
Table 4: Paternal age in cytogenetically analyzed cases
|
S. No |
Cytogenetics of Down syndrome cases |
(%)age of cases |
Age of father (years) |
| 1 | Free trisomy 21 | 94.5 | 20-46 |
| 2 | Translocation 14; 21 | 1.1 | 34 |
| 3 | Mosaic for translocation 21; 21 | 1.1 | 35 |
| 4 | Mosaic for free trisomy 21 | 1.1 | 37 |
| 5 | Normal cytogenetics with | 2.2 | 30-35 |
| Down syndrome phenotype |
Table 5: Cytogenetics of Down syndrome cases and paternal age (<30 years and >30 years)
|
Cytogenetics |
<30 years Father |
>30 years Father |
|
Free trisomy 21 |
(24.71%) |
(75.29%) |
| Translocation 14; 21 | – | 1.1 |
| Mosaic trisomy 21 | –‘ | 1.1 |
| Mosaic translocation 21;21 | – | 1.1 |
| Normalcytogenetics with Down syndrome phenotype | – | 3.1 |
| Total | (32.3%) | (76.7%) |
Table 6: Paternal age in free trisomy 21 cases.
| Parental age | Down syndrome cases (years) | (%) Father |
| 20-25 | (2.36%) | (24.71%) * |
| 26-30 | (22.35%) | |
| 31-35 | (41.47%) | |
| 36-40 | (22.35%) | (75.29%)** |
| > 40 | (11.76%) |
* Age below 30
** Age above 30
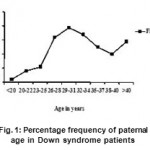 |
Figure 1: Percentage frequency of paternal age in Down syndrome patients.
|
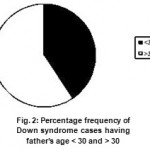 |
Figure 2: Percentage frequency of Down syndrome cases having father’s age < 30 and > 30.
|
Discussion
The only etiological factor that has been established in literature is advanced maternal age for the occurrence of trisomy 21 (Penrose 19339; Hassold and Sherman 200010; Petersen and Mikkelsen 200011). The question whether there is a paternal age effect on male nondisjuction remains uncertain. The analysis of Down syndrome patients in the present study depicted that mean paternal age was 31.5 years for Down syndrome cases. Variability in age of father was found from 19 years to the 48 years at the birth of mongoloid child. Down syndrome cases born to father of less than 30 years of age were 40.5% while those born to more than 30 years of age were 59.5%. The existence of a pater nal age effect on Down syndrome is controversial. Various Down syndrome studies from United States and Europe showed no influence between paternal age and Down syndrome (Regal et al 198012; Ferguson-Smith and Yates 198413; Erickson and Bjerkedal 198114; Roth et al 198315). Contrary to this, a Canadian study of 997 cases of Down syndrome revealed a increasing rate of Down syndrome cases with increasing paternal age (McIntosh et al 199516). According to one study paternal age is considered without the interaction of increased maternal age (and vice versa), no apparent relationship between paternal age and Down syndrome was found therefor it is reasonable to assume a positive correlation between maternal age and paternal age (Harry et al 200317).
Pater nal age was dismissed by the Penrose (19339) as insignificant in the etiology of Down syndrome but controversy over this point continued, mainly because equivocal data could not be obtained either suppor ting or rejecting it (Carothers 198818; Hook and Cross 199019). Neither is there convincing evidence for a paternal age effect for trisomic abortuses (Hatch et al. 199020). Present study depicted a positive statistical value of correlation coefficient for father’s age. Use of heteromorphic chromosome banding had indicated that fathers contribute the extra chromosome in 15- 20% of Down syndrome children (Del Mazo et al 198221; Juberg and Mowrey 198322; Antonarakis et al 199123). Although meiotic nondisjunction is undoubtedly the cellular malfunction those results in free trisomy. Some interrelated and challenging questions regarding basic mechanism of nondisjunction & paternal age are still unanswered.
The compromised microcirculation hypothesis explains the occurrence of aneuploidy in primary and secondary oocytes, sperm precursor cells, tumor and embryonic cells. Generally older wives tend to be married to older husbands. Therefore it is not immediately obvious whether an increased risk with parental age can be traced to fathers, mothers or both parents. In Down syndrome, Penrose (1933)9 showed the increase in risk to be exclusively due to the mother’s age. Epidemiological studies have identified many candidates for extrinsic factors including smoking, alcohol, maternal irradiation, fertility drugs, oral contraceptives and spermicides. However an equivocal proof is still lacking for these as well as other intrinsic and extrinsic factors. Present study showed a little bit positive correlation between paternal age & incidences of Down syndrome but not up to significant level, it may be due to combined
effect of advanced parental age or may be due to environmental and genetic factors. Such data would also be helpful in better assessment of the environmental factors (physical, biological, chemical, mutagens) and genetic factors that have been considered as possible causes for Down syndrome. Although more research is needed to confirm these findings, & father’s age should not be ignored while studying genetic abnormalities. With the advent of the DNA polymorphic markers the effect of paternal age on Down syndrome can be more clearly depicted.
Acknowledgements
The authors are thankful to Arpan Institute of Mentally retarded children, Rohtak, & other rehabilitation institutes of Haryana, the parents & guardians for providing kind co-operation & information. We are also thankful to UGC for JRF & ICMR for providing SRF (Senior Search Fellowship) & major research project grant.
References
- Down, J.H. Observations on an ethnic classification of idiots. In Clinical Lecture reports. London Hospital. 3: 259-262(1866).
- Kotzot, D. and Schinzel, A. A. Paternal meiotic origin of der (21;21) (q10;q10); mosaicism [46,xx/46,xx, der (21;21) (q10;q10); +21] in a girl with mild Down syndrome. Eur J Hum Genet, 8: 709-712 (2000).
- Pangalos, C., Avramopoulos, D., Blouin, J. , Raoul, O., De Blois, M. C. and Prieur, M. Understanding the mechanism(s) of mosaic trisomy 21 by using DNA polymorphism analysis. Am J Hum Genet, 54: 473-481 (1994).
- Vashist, , Neelkamal, Yadav, R. and Lal,
- M. Trisomy-T(21;21)with mosaicism in a Down syndrome girl Case Report. Int J Hum Genet, 9(2): 15-107 (2009).
- Kaur, A. and Singh, R. P. Chromosomal Abnormalities: Genetic Disease Burden in India. Int J Hum Genet, 10(1-3): 1-14 (2010).
- Fox, D. and Sindwani, V. SatelliteKaryogram, 11: 3(1985).
- Ghalib, M. and Isaac, G. S. Paternal consanguinity in Down syndrome. Ann Natl Acad Med Sci (India), 27: 43-46 (1991).
- Shi, Q. and Martin, R. H. Aneuploidy in human sperm: a review of the frequency and distribution of aneuploidy, effect of donor age and life style factors. Cytogenet Cell Genet, 90: 219-226 (2000).
- Penrose, L. S. The relative effects of paternal and maternal age in J. Genet, 27: 219-224 (1933).
- Hassold, T. & Sherman, S. Down syndrome: genetic recombination and the origin of the extra chromosome 21. Clin Genet, 57: 95- 100 (2000).
- Petersen, M. B. and Mikkelsen M. B. Nondisjunction in trisomy 21: origin and Cytogenet Cell Genet, 91: 199- 203 (2000).
- Regal, R. , Cross, P. K., Lamson, S. H. and Hook, E. B. A search for evidence for a pater nal age effect independent of a maternal age effect in birth certificate reports of Down’s syndrome in New York State. Am J Epidemiol, 112 (5): 650-655 (1980).
- Ferguson-Smith, M. A. and Yates, J. Maternal age specific rates for chromosome aberrations and factors influencing them: report of a collaborative European study on 52, 965 amniocenteses. Prenat Diagn, 4: 5- 44(1984).
- Erickson, J. D. and Bjerkedal, T. Down syndrome associated with father’s age in Norway. J Med Genet, 18 (1): 22-28(1981).
- Roth, M. P., Stoll, C., Taillemite, J. , Girard, S. and Boue, Paternal age and Down’s syndrome diagnosed prenatally: no association in French data. Prenat Diagn, 3: 327-335 (1983).
- McIntosh, C., Olshan, A. F. and Baird P. Paternal age and the risk of birth defects in offspring. Epidemiology, 6: 282-288 (1995).
- Fisch, , Hyun, G., Golden, R., Hensle T. W., Olsson, C. A and Liberson, G.L. The influence of pater nal age on Down Syndrome. The Journal of Urology, 169: 2275–2278 (2003).
- Carothers, D. Controversy concerning pater nal age effect in 47, + 21 Down syndrome. Hum Genet, 78: 384-385 (1988).
- Hook, E. B. and Cross, P. Factual statistical and logical issues in the search for paternal age effect for Down syndrome. Hum Genet, 85: 387-388 (1990).
- Hatch, , Kline, J., Levin, B., Hutzler, M. and Warburton D. Paternal age and trisomy among spontaneous abortions. Hum Genet, 85: 355-361 (1990).
- Del Mazo, J., Castillo, A. P.and Abrisquenta, J.S.Trisomy 21: origin of nondisjunction. Hum Genet, 62: 316-320 (1982.)
- Juberg, R. C. and Morwey, P. Origin of nondisjunction in trisomy 21 syndrome: all studies compiled, parental age analysis and international comparisons. Am J Med Genet, 16: 111-116 (1983).
- Antonarakis, S.E. Down syndrome due to de novo robertsonian translocation t(14;21) polymorphism suggests that the origin of extra 21q is maternal. Am J Hum Genet, 49: 529-536(1991).

This work is licensed under a Creative Commons Attribution 4.0 International License.



