

How to Cite | Publication History | PlumX Article Matrix
Air Pollutions Triggering Myocardial Infarctions based on Diagnosis with CK-MB Levels
A. Julius, S. Raghavendra Jayesh and V. Saravanan
Department of Biochemistry, Sree Balaji Dental College and Hospital, Bharath University of Higher Education and Research, Narayanapuram, Pallikaranai, Chennai - 600 100 India.
ABSTRACT: This study indicates that there is a direct relationship between AMI and pollution that is the number of admissions with AMI to the hospital is directly proportional to increase in pollution.
KEYWORDS: AMI (Acute Myocardial infarction); CK-MB(Creatine kinase-myocardium)
Download this article as:| Copy the following to cite this article: Julius A, Jayesh S. R, Saravanan V. Air Pollutions Triggering Myocardial Infarctions based on Diagnosis with CK-MB Levels. Biosci Biotech Res Asia 2011;8(2) |
| Copy the following to cite this URL: Julius A, Jayesh S. R, Saravanan V. Air Pollutions Triggering Myocardial Infarctions based on Diagnosis with CK-MB Levels. Biosci Biotech Res Asia 2011;8(2). Available from: https://www.biotech-asia.org/?p=9838 |
Introduction
The myocardium is composed of specialized cardiac muscle tissue found only in the heart.(Ross et al). Cardiac muscles are auto rhythmic that is they can contract on their own in a slow, steady rhythm. Because the muscular myocardium can contract powerfully and rhythmically, the heart is an efficient pump for blood (Garry et al).
According to the World Health Organization (WHO), the definition of acute Myocardial Infarctions includes the presence of two of the following three criteria, 1.Characteristic chest pain usually for more than 20 minutes. 2. Diagnostic ECG Changes 3.Rise and subsequent fall of the serial levels of cardiac bio-chemical markers.
These cardiac markers (specifically CK-MB) play an important role in the detection of acute myocardial infarctions especially in the group of patients with low to medium risk and minor myocardial injury and most useful when individuals have non – diagnostic ECG tracings (William et al).
An infarct is an area of tissue that has died because of lack of oxygenated blood. The myocardium is affected when a branch of a coronary artery is occluded.(Ross et al). Occlusion of a coronary artery by lipids deposits can cause severe local oxygen starvation and ultimately the degeneration of a localized portion of the heart muscle, this process called as AMI. Measurement of the concentration of the two aminotransferase in the blood serum by the SGPT and SGOT tests and other heart enzyme CK test can provide information about the severity and the stage of the damage to the heart (Garry et al). CK is the first enzyme to appear in the blood after AMI (Lehniger et al). This Myocardial injury is caused by various factors. Apart from them the air pollutions are also triggering the AMI (Anette Peters et al).
The WHO defines air pollution “the presence of materials in the air in such concentration which are harmful to man and his environment. In fact air pollution is the occurrence or addition of foreign particles, gases and other pollutants into the air which have an adverse effect on human beings.
The Major sources of air pollutions are Stationary combustion sources; these include products of burning fuel by people and Mobile combustion sources; these include locomotives, automobiles, air craft etc. An elevated concentration of the air pollutants triggers the AMI in the population, which live for a long period of time to air pollution exposure. Even transient exposure to traffic may increase the risk of myocardial infarction in susceptible persons. In addition even changes from moderate to heavy air pollution were associated with an increased risk of AMI (Rosenlund et al).
The factors that govern carbon monoxide toxicity include CO’s concentration levels in the inspired air, duration of exposure and the general health of the person. Old people and those with cardio-respiratory diseases are more at risk. Anyone who inhales the gas in concentrated form suddenly turns pale, weak and dizzy, leading to coma and death due to respiratory failure. When carboxyhaemoglobin is formed, the skin and the mucous membrane turn cherry red, indicating the severity of poisoning. (Truman’s and Wahoid et al).
This study is designed to assess the extent to which the exposure to pollutions caused by vehicular traffic can trigger myocardial infarctions on the basis of the cardiac biochemical marker as CK-MB levels. Creatine kinase (Creatine phosphokinase (or) adenosine triphosphate; Creatine N-Phosphotransferase) is a dimeric enzyme that catalyses the reversible phosphorylation of Creatine. Human tissues have shown to contain three cytosolic enzymes for CPK. They are CPK1, CPK2 and CPK3. Each of the CPK enzymes is a dimmer. The CPK enzymes are separated by using electrophoresis and Ion-exchange chromatography methods (Tietz et al and D.J.Anderson et al).
CPK1 contains two polypeptide chains (BB) found in brain (CKBB)
CPK2 contains two polypeptide chains (MB) found in myocardium (CKMB)
CPK3 contains two polypeptide chains (MM) found in Skeletal
Muscles (CKMM).
CK-MB has become the “gold standard” for the diagnosis of AMI. Because it is more specific for the myocardium, which contains 10-20% of the total activity as CK-MB compared with less than 2% of the total activity of CK-MB in skeletal muscles.
The activity of CK-MB is increased in AMI and circulated in the blood within 3-6 hours. The activity of CKMB is more sensitive indictor in the early stages of AMI. It is also present in skeletal muscle in low amounts only about less than 2% of the total CK activity (William et al, M.N. Chaterjee, and Pant).
In patients with acute myocardial infarction the activity of creatine kinase isoenzyme MB in plasma consistently accounts for 15% of the total CK activity. By contrast, the CKMB content of cardiac tissue, although sometimes reported to be consistent with the 15% plasma activity of CKMB has also been reported to be negligible in healthy myocardium. (Marie-Louise L. Boumans et al). Normally CK-MB is very small in amount and represents only about 2% of the total serum CK. However in AMI it may increase upto 20% of the total serum CK activity with in 4 hours (William et al, pant, Chaterjee).
Materials and Methods
Seventy eight subjects were studied with AMI in heavily and moderately polluted areas, which was compared with the same age and sex, matched 18 controls. Their CK-MB activity was assayed by the method of Szasz et al. Modifications of this formulation, particularly in regard to buffer and adenylate kinase inhibitors, have also been introduced.
Results and Discussion
The study group included 36 patients in moderately polluted areas (age ranging from 45 to 70 years ) and 42 patients in heavily polluted areas (age ranging from 45 to 75 years). The control group consisted of 18 members (age ranging from 45 to 70 years).
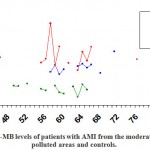 |
Figure 1: CK-MB levels in Moderately polluted areas(MPA) and in Heavily polluted areas (HPA)compared with the controls. |
Table 1: CK-MB levels of patients with AMI from the moderately & heavily polluted areas and controls.
| Particulars | Control | MPA | HPA |
| CK-MB | 1.4±0.38
(n=18) |
2.2±0.46
(n=36) |
4.2±0.85
(n=42) |
X –axis-indicates the % of CK-MB
Y-axis- indicates Age
MPA- Moderately polluted areas
HPA- Heavily polluted areas
The percentage activity of CK-MB values did not increase (<10% of activity) in any person in the control group. The peak ranged from minimum 2.8 % to maximum 7.6 %. In case of patients in moderately polluted areas the percentage activity of CK-MB levels were increased than that of the controls. The percentage activity of CK-MB ranged from 10 to 20 %. The minimum was 10.8 % and the maximum was 18.8 %. In heavily polluted areas the percentage activity of CKMB levels were found to be significantly when compared to that of the controls. The percentage activity of CK-MB increased up to 30%. The peak value of minimum was found to be 14.1% and the maximum was found to be 28.7 %. The patients with AMI, showed various symptoms namely severe chest pain more than 20 minutes nausea, shortness of breath and dizziness. Myocardial ischemia is the prior stage of AMI in which obstruction of a coronary artery leads to severe oxygen deprivation of the myocardium. The major causes of AMI are the atherosclerotic plane rupture and thrombus formation. Apart from the factors mentioned above ‘Air Pollution’ adds to the increase in AMI.
We compared moderately polluted area with the heavily polluted area. The percentage activities of CKMB levels were increased depending on the degree of pollution as shown below in the graph.
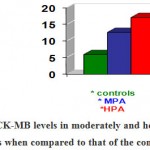 |
Figure 2: CK-MB levels in moderately and heavily polluted areas when compared to that of the controls. |
CK-MB levels in the heavily polluted areas showed very high significance when compared to that of the controls and CK-MB levels in the moderately polluted areas were found to be significantly increased when compared to that of the controls.
Summary
The present study suggests that an elevated concentration of air pollution increase the risk of AMI for the people who live in continuous exposure for a long term in the particular polluted areas. In the admission of the patients with AMI, to the hospital the diagnosis is made with reference to the percentage of activity of CKMB levels. On a comparison, the percentage of CKMB activity in the population between the moderately and heavily polluted areas, the population in the heavily polluted areas has high percentage of CKMB activity. Because of the exposure to the pollutants namely CO, SO2, NO2, particulate matter etc, the concentration of which increased in day to day emission, there was an increase in the admission of the patients with AMI to the hospital. With in the ambit of this project, the increase in the percentage of CKMB levels due to an increase in the air pollution caused exclusively by the emission of exhaust by the vehicular traffic could not be fully studied. This aspect can be studied in a further detailed research project.
References
- Annette Peters Ph.D, Douglas W-Dockery SCD James E-Muller, MD; Murray A Mittleman MD Dr PH – Jun-2001. Clinical investigation and reports increased particular air pollution and the triggering of myocardial infarctions.
- Chatterjea M.N. , Rana Shinde, 3rd edition Teatbook of Medical biochemistry
- Garry A- Thibodeau, Kevin T-Palton Anthony’s Text book of Anatomy and Physiology 4th edition
- Lehninger, Nelson, Cox, Principles of Bio-Chemistry 2nd editions
- Marie-Louise L. Boumans, Jart H.C. Diris, Marius Nap, Arno M.M. Muijtjens, Jos G. Maessen, Marja P. van Dieijen-Visser Wim T. Hermens. Creatine Kinase Isoenzyme MB (CKMB) Controversy: Perimortal Tissue Acidosis May Explain the Absence of CKMB in Myocardium at Autopsy
- Pant M.C. 9th Essential of biochemistry.
- Rosenlond – M, berglind N, Pershagon G, Hallavist J, Jonson T, Bellander T in July-2006. Long-term exposure to urban air pollutions and myocardial infarction.
- Ross and Willson anatomy and physiology in health illness 8th
- Tietz, Carl-A-Burtis, Edward R-Ashwood 5th Fundamentals of clinical chemistry.
- Trueman’s VGG/CSIR (JRF/NET) specific for life science – pramod singh 1st edition 2004.
- Varley’s practical clinical Biochemistry Alan-H-Gowenlock 6th
- Willam W, Chu, MD, Ph.D., Robert S. Dieter MD; Charles K. Stone MD. Wislonsin Medical Journal – 2002. A Review of clinically relevant cardiae biochemical markers
- Wahoid U-Malik G.D, Tuli R.D Madan 7th Selected topic in inorganic chemistry.

This work is licensed under a Creative Commons Attribution 4.0 International License.



