

How to Cite | Publication History | PlumX Article Matrix
Acute Lymphocytic Leukemia: An epidemiological and Hematological Study from Haryana
Ashok Kumar1, Radha Rathee1, Minakshi Vashist1, Neelkamal, Sunita Singh 2and Sumiti Gupta2
1Department of Genetics, M.D.University, Rohtak, Haryana, India.
2Department of Pathology, Pt.B.D. Sharma University of health Sciences, Rohtak, Haryana, India.
Corresponding Author E-mail: mvashist@rediffmail.com
DOI : http://dx.doi.org/http://dx.doi.org/10.13005/bbra/1069

ABSTRACT:
Patients diagnosed with acute lymphocytic leukemia (ALL) were evaluated to characterize epidemiological and hematological studies. 94 patients of Acute Lymphocytic Leukemia were included in present study for parameters like age of diagnosis, sex, occupation, prenatal and postnatal history and hematological analysis. Out of 94 patients, there were 70.2% children and 29.8% adults. Children patients were maximum in age group of 6-10 years whereas adult patients were maximum in age group of <20 years. There were more males than females in children as well as adults except age group 41-50 years where females were more than males. B-cell ALL was more frequently observed than T-cell ALL in children as well as adults. Drug intake was major risk factor during pregnancy and smoking was major risk factor after birth. Agriculture was major occupation in Parents of children as well as adults. Maximum patients had W.B.C count less than 50X109/L and hemoglobin more than 10 gm/100ml.
KEYWORDS: Acute lymphocytic leukemia; Epidemiology; Risk factors.
| Copy the following to cite this article: Kumar V, Rathee R, Vashist M, Neelkamal, Singh S, Gupta S. Acute Lymphocytic Leukemia: An epidemiological and Hematological Study from Haryana. Biosci Biotech Res Asia 2012;9(2) |
| Copy the following to cite this URL: Kumar V, Rathee R, Vashist M, Neelkamal, Singh S, Gupta S. Acute Lymphocytic Leukemia: An epidemiological and Hematological Study from Haryana. Biosci Biotech Res Asia 2012;9(2). Available from: https://www.biotech-asia.org/?p=10140 |
Introduction
Acute lymphoblastic leukemia (ALL) is a type of leukemia which is characterized by the overproduction and continuous multiplication of malignant and immature lymphocytes (Lymphoblast) in the bone marrow. The worldwide annual incidence of acute lymphoblastic leukemia is approximately 9-10 cases per 100,000 populations in childhood1. The ALL arise from B-cell in 85% patients and from T-cell in 15% cases. In children, B-cell acute lymphocytic leukemia accounts for 60-80% cases whereas T-cell comprises only 11-20%2. Approximately 3/4 of all cases of childhood leukemia are acute lymphoblastic leukemia. About 3,000 children in the United States and 5,000 children in Europe are diagnosed with ALL each year. The age-adjusted incidence of ALL in adults (usually defined as 15 years of age and older) amounts to about one third of that in children. Acute lymphoblastic leukemia occurs slightly more frequently in males than in females. The etiology of ALL remains uncertain, although some doctor believes that ALL develop from a combination of genetic and environmental factors. The causative factors may be like smoking, high birth weight, diet, high socioeconomic status, electromagnetic field, being exposed to radiation, pesticides, past treatment with chemotherapy or other drugs that weaken the immune system. Similarly certain changes in genes or genetic disorders, such as Down syndrome and maternal alcohol consumption may be considered as predisposing factors for ALL3,4. There is limited data available on epidemiology, clinical and laboratory features of ALL from Haryana. So an attempt was made to know the epidemiology of ALL patients from Haryana.
Patients and Methods
The study was carried out on 94 patients of acute lymphocytic leukemia registered in Pt. B.D. Sharma University of health sciences, Rohtak. A detailed Performa was filled in for patients especially regarding age, sex, occupation, and education, family history of patients and their parents, clinical finding, prenatal and postnatal history of patients. Patients were divided into two categories children (<15 years) and adults (>15 years). Age and sex specific distribution of patients was done separately in children and adults. Out of 94 patients, 77 (50 children, 27 adults) of newly diagnosed acute lymphoblastic leukemia (ALL) were included for hematological analysis. The blood samples of patients were analyzed for W.B.C count and hemoglobin concentration. W.B.C. count was done using hemocytometer and hemoglobin was measured by hemometer. Number of W.B.C was calculated and divided into three groups viz <50X109 /L, 50-100X109/L & >100 X109/L. Similarly amount of hemoglobin was measured and divided into three groups viz < 5 gm/100ml, 6-10 gm/100ml & >10 gm/100ml.
Results
In the present study there were 70.2% children and 29.8% adults. In children, maximum patients were in age group of 6-10 years followed by 2-5 years, 11-15 years & < 1 year (Figure-1). Adult patients had maximum cases in age group of <20 years, and lowest in age group of 41-50 years. There was no patient in age group 51-60 years (Figure-2). There were 67% males and 33% females; male to female ratio was 2.03:1. Males were more than females in all age group of children and adults except age group 41-50 years where females were more than males (Figure-3 & 4). B-cell ALL were found in 85.1% patients and T-cell ALL in 14.9% patients. There were 81.8% B-cell and 19.2% T-cell ALL in children however adult had 92.8% B-cell and 7.2% T-cell ALL patients (Figure-5).
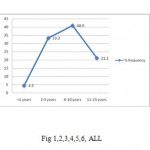 |
Figure 1,2,3,4,5,6: ALL
|
Various risk factors considered in the present study were categorized as drug intake, smoking, alcohol consumption, pesticides exposure, ionizing radiation exposure, electromagnetic field, infection & fetal loss. The drug intake was a risk factor in 44.4 % followed by fetal loss 14.2%, pesticides 11.1% and exposure to ionizing radiation 3.8%. Smoking was risk factor in 16.8% patients followed by exposure to ionizing radiation 15.5%, pesticides 12.9%, alcohol consumption 11.6%, infection 10.3% and electromagnetic field 6.4%. Alcohol consumption was a risk factor only in adults. The agriculture was an occupation in 44.2% patients. 22.3% were engaged in different Industries and 13.8% patients and their parents were business man. Nineteen percent patients and their parents were workers in unorganized sector. Farmers and business man were slightly more in adults as compared to children however industrial workers and labour had more frequency in children than adults.
W.B.C count at diagnosis was less than 50X109 /L in 48% patients, between 50-100 X109/L in 31% patients and more than 100 X109/L in 21% patients. W.B.C count was less than 50X109 /L in 50% children and in 44.4% adults, between 50-100 X109/L in 26% children and in 40.7% adults, and with more than 100 X109/L in 24% children and in 14.8% adults (Figure-6).
Hemoglobin was less than 5gm/100ml in 19% patients, 6-10 gm/100ml in 34% patients and more than 10gm/100ml in 47% patients. Hemoglobin was less than 5gm/100ml in 24% children and in 11.1% adults, between 6-10 gm/100ml was in 30% children and in 37.3% adults, more than 10 gm/100ml in 46% children and in 51.8% adults.
Discussion
Acute lymphoblastic leukemia, the most common childhood acute leukemia, represents about 80% of acute leukemias; however, it makes up only 20% of adult leukemias. In present study, there were 70.2% children and 29.8% adults from Haryana. The relative contribution of leukemia to the total childhood cancer burden varies markedly with age, being 17% in the firs year of life, increasing to 46% for 2 and 3 years olds, and then decreasing to only 9% for 19 year old5. The age distribution of children of ALL in developed countries shows a very marked early peak between 2-5 years, followed by a small peak between 11-15 years and the median age of 4 years6,7.8. The incidence of ALL among 2-3 years old is approximately 4-folder greater than that for infant and is nearly 10-fold greater than that for 19 year olds9 among adults, it is somewhat more common in people older than 45. The incidence of ALL has increased from 0.39/100000 in adult aged 35-39 years to 2.1/100000 in patients above 85 years10. Moorman et al have reported higher frequency of adults in age group of 15-19 years11. The majority of patients in the present study were in the age group of 11-15 years with a male predominance, followed by a second peak between 2-5 years which is apposite to western population. Among adults, higher frequency was in age younger than 20 years but patients were less frequently observed in other age groups.
Incidence of ALL has been recorded 30% higher in males as compared to females in the literature3,12,13. The male to female ratio was 1.3:1 in children of acute lymphocytic leukemia in developed countries6,7,8. In India, the reported incidence of childhood cancer in male is higher than in females in all PBCRs except in North East India. The male to female ratio was 2.03:1 in patients of acute lymphocytic leukemia in present study that is much higher than what is seen in the developed world. Moorman et al have reported more males than females in all group of a population based study11.
B-cell acute lymphocytic leukemia was found in 60-80% of children whereas T-cell compromised only 11-20%2,14. There were reports of higher frequency of B-cell than T-cell in the elderly population15,16,17. In the present study, B-cell ALL was observed more frequently in children as well as in adult patients. However a lower incidence of B-cell ALL have been reported from India18,19.
The drug intake was a major prenatal risk factor followed by fetal loss, pesticides and exposure to ionizing radiation. The risk factor like drug intake, pesticides exposure and fetal loss were more in children than adults. Smoking was a major postnatal risk factor followed by pesticides, exposure to ionizing radiation, alcohol consumption, electromagnetic field and infection. Alcohol consumption was a risk factor only in adults. Various prenatal and postnatal factors similar to present study have been reported in literature20,21,22,23.
W.B.C count at diagnosis was less than 50X109 /L in 48% patients, between 50-100 X109/L in 31% patients and more than 100 X109/L in 21% patients. Hemoglobin was more than 10gm/100ml in 47% patients followed by 6-10 gm/100ml (34%) & less than 5 gm/100ml (19%). Higher hemoglobin has been reported to denote poor prognosis in western series24,25 however data from India has shown lower Hb associated with worse prognosis26.
Conclusion
Acute Lymphocytic leukemia was more commonly observed in children than adults. Maximum patients were in age group of 6-10 years and <20 years. Males were more frequently observed than females. B-cell was more commonly observed than T-cell. Drug intake was major risk factor during pregnancy and smoking was major risk factor after birth. Maximum patients had W.B.C count less than 50X109 and hemoglobin more than 10gm/100ml followed by 6-10 gm/100ml & less than 5 gm/100ml. This study will be helpful in defining the risk category of patients. We believe that further studies with larger sample sizes will shed light on the prognosis and treatment of ALL, and this condition ought to be evaluated in prognosis of leukemia.
Acknowledgment
We would like to express gratitude to Dr. Sunita Singh Prof. Deptt. of Pathology, Dr. Pankaj Abrol, Head, Deptt. of Paedeatics and Dr. Gahlot, Head, Deptt of Medicine Pt. B. D. Sharma University of Health Sciences, Rohtak for the cooperation and help in collecting data. I express my sincere thank to UGC for funding this project.
References
- Ribera, J.M., Oriol, A. Acute lymphoblastic leukemia in adolescents and young adults. Hematol Oncol Clin North Am, 2009; 23(5): 1033-42, vi.
- Greaves, M.F., Janossy, G., Peto, J., et al. Immunological defined subclass of acute lymphoblastic leukemia in children relationship to presenting features and prognosis. Br J Haemat, 1981; 48: 179.
- Sandler, D.P., Ross, J.A. Epidemiology of acute leukemia in children and adults. Semin Oncol, 1997; 24: 3-16.
- Ross, J.A., Potter, J.D., Shu, X.O., et al. Evaluating the relationships among maternal reproductive history, birth characteristics, and infant leukemia: a report from the Children’s Cancer Group. Ann Epidemiol, 1997; 7:172-9.
- Margolin, J.F., Poplack, D.G. Acute Lymphoblastic Leukaemia. In Pizzo P.A., Poplack D.G., editors. Principles and practices of pediatric oncology. Philadelphia: Lippincott Raven, 1997; pp 409-63.
- Hanson, M.R., Mulvihill, J.J. Epidemiology of child-blood cancer. In Levine A.S., ed Cancer in the Young. NewYork: Masson, 1980; pp 3-12.
- Draper, G.J., Kroll, M.E., Stiller, C.A. Childhood Cancer. Cancer Surv, 1994; 307: 493-517.
- Gurney, J.G., Daris, S., Severson, R.F., Fang, J.Y., Ross , J.A., Robinson, L.L. Trends in Cancer incidence among children in US. Cancer , 1996; 78: 532-41.
- Smith, A.J.H., De Sousa, M.A., Kwabi-Addo, B., Heppell-Parton, A., Impey, H. and Rabbitts, P.H. A site-directed chromosomal translocation induced in embryonic stem cells by Cre-loxP recombination. Nature Genet, 1995; 9: 376–384.
- Amino, L., Goekbugot, N., Delannoy, A. Acute lymphocytic leukemia in the eldery. Hematol J 2002; 3: 219-223.
- Moorman, A.V., Chilton , L., Wilkinson, J., Ensor, H.M., Bown, N., Proctor, S.J. A population-based cytogenetic study of adults with acute lymphoblastic leukemia. Blood, 2010;115(2): 206–214.
- Ross, J.A., Davies, S.M., Potter, J.D., Robison, L.L. Epidemiology of childhood leukemia with a focus on infants. Epidemiol Rev, 1994; 16: 243–272.
- Robinson, H.M., Taylor, K.E., Jalali, G.R., Cheung, K.L., Harrison, C.J. & Moorman, A.V. t(14;19)(q32;q13): a recurrent translocation in B-cell precursor acute lymphoblastic leukemia. Genes, Chromosomes and Cancer, 2004; 39, 88–92.
- Greaves, M.F., Alexander, F.E. An infectious etiology for common acute lymphoblastic leukemia in childhood? Leukemia, 1993; 7(3): 349–360.
- Taylor, P.R.A., Reid, M.M., Proctor, S.J. Acute lymphoblastic leukemia in the elderly. Leuk Lymphoma, 1994;13: 373-380.
- Kantarjian, H.M., O’Brien, S., Smith, T.L., et al. Results of treatment with hyper-CVAD, a dose-intensive regimen, in adult acute lymphocytic leukemia. J Clin Oncol, 2000; 18: 547-56.
- Gokbuget, N., Arnold, R., Buechner, Th., et al. Intensification of induction and consolidation improves only subgroups of adult ALL: Analysis of 1200 patients in GMALL study 05/93 [abstract]. Blood, 2001; 98: 802a.
- Bhargava, M. Kumar, R. Karak, A. et al. Immunological subtypes of acute lymphoblastic leukemia in North India. Leuk Res, 1998; 12: 673-78.
- Rajalekshmy, K.R., Abitha, A.R., Pramila, R., Gnanasagar, T., Maitreyan, V., Shanta, V. Immunophenotyping of acute lymphoblastic leukaemia in Madras, India. Leuk Res, 1994; 18: 183-90.
- Shu, X.O., Gao, Y.T., Brinton, L.A., et al. A population- based case-control study of childhood leukemia in Shanghai. Cancer, 1988; 62: 635-44.
- Savitz, D.A., Wachtel, H., Barnes, F.A., et al. Casecontrol study of childhood cancer and exposure to 60-Hz magnetic fields. Am J Epidemiol, 1988; 128:21-38.
- Schmitz-Feuerhake, I., Dannheim, B., Heimers, A., Oberheitmann, B., Schroder, H., Ziggel, H. Leukemia in the proximity of a German boiling-water nuclear reactor: evidence of population exposure by chromosome studies and environmental radioactivity. Environmental Health Perspectives, 1997; 105 Suppl 6:1499-504.
- Brondum, J., Shu, X.O., Steinbuch, M., Severson, R.K., Potter, J.D., Robison, L.L. Parental cigarette smoking and the risk of acute leukemia in children. Cancer, 1999; 85:1380–1388.
- Steinherz, P.G., Siegel, S.E., Bleyer, W.A., Kersey, J., Chard, R., Coccia, P., et al. Lymphomatous presentation of childhood acute lymphoblastic Leukaemia. A subgroup at high-risk of early treatment failure. Cancer, 1991; 68: 751-8.
- Steinherz, P.G., Gaynor, P.S., Breneman, J.C., Cherlow, J.M., Grossman, N.J., Kersey, J.H., et al. Treatment of patients with acute lymphoblastic Leukaemia with bulky extramedullary disease and T-cell phenotype or other poor prognostic features: Randomized controlled trial for the Children’s Cancer Group. Cancer, 1998; 82: 600-12.
- Advani, S.H., Malhotra, H., Kadam, P.R., Lyer, R.S., Nanjangud, G., Balsara, B., Saikia, T., Gopal, R., Nair, C. T-Lymphoid blast crisis in chronic myeloid leukemia. Am J Hematol, 1991; 36: 86-92.

This work is licensed under a Creative Commons Attribution 4.0 International License.



